◀هل اللقاح ضروري❓ هل يفيد صحتنا❓ هل اللقاح يعتمد المعيار الأخلاقي❓ ماذا عن الفعالية ❓
◀ العالمة “Pamela Acker”: بعض لقاحات “الكورونا” معدّ على طريقة الأزتيك ❓
◀ الدكتورة تيريزا ديشر Dr. Theresa Deisher من شركة Sound Choice Pharmaceuticals.. لها أعمال هائلة وقد لخصت الكثير منها عَ YouTube هناك علاقة بين زيادة استخدام اللقاحات المشتقة من الخلايا جنينية مُجهضة والتي تتوافق مع زيادة معدلات التوحد.. لقاحات الخلايا الجنينية المجهضة التي نستخدمها ، تزداد حالات التوحد.. ينتهي بك الأمر بفقدان الحمض النووي الفعلي ودمج الحمض النووي من الخلايا الجنينية المجهضة في خلاياك.. 😎
◀ هل من احتيال علمي بخلايا “HEK-293 التي هي كلية جنينية بشرية.. وهل من عوارض ❓
◀ ما إن عبّرت عام 2010 عن مخاوفي طُردت من المعمل الناشط بتطوير اللقاحات والممول من مؤسسة Bill & Melinda Gates.. 😎
◀ ما هو HEK-293 بالضبط؟
◀ ماذا عن العملية المُسمّاة “بخلايا الخلود” وما يُحكى عنه ويهلّل له “أنه يلقحون بخلايا تعيش إلى الأبد” في المختبر. يمكنها جعلهم يعيشون لفترة أطول من الخلايا الأولية.. كأن تأخذ شيئًا من ذراعي وينمو في طبق بتري.. ولكن ليس كثيرًا.. غالبًا ما تُعطى سلالات الخلايا الخالدة جينات معززة للسرطان بتعطيل وظيفة الجينات الكابتة للسرطان أو االكابتة للورم. وهكذا يمكن أن يكون لديك عمر افتراضي أقصر..😎 وعندما تحصل على اللقاح أنت في الواقع تحقن أجزاء من هذا الشخص الذي قُتل في جسمك. وهذه القطع تميل إلى أن تكون بقايا الحمض النووي وبعض حطام البروتين.. ⛔
◀ لو نتحدث عن إجهاض تلقائي إن هذا الطفل يموت قبل وقت طويل من إزالة أنسجة الجنين.. أسوأ من ذلك بكثير.. الأطفال على قيد الحياة معذبّة عندما يبدأ الباحثون في استخراج الأنسجة..
◀ تمّ إزالة الكيس الأمنيوسي بالكامل من الأم وتم تشريح هؤلاء الأطفال 😎
◀ الحصبة الألمانية نفسها ليست مرضًا خطيرًا إذا تم التقاطه بمرحلة الطفولة، معظم الناس لن تظهر عليهم أعراض. ولكن بالسنوات العشر الأولى بعد تقديم اللقاح لا انخفاض بل ارتفاع في حالات متلازمة الحصبة الألمانية الخلقية ولم يبدأ بالانخفاض حتى أصبح الإجهاض قانونيًا. (للتخفيف من نسبة أرقام الوفيات) فلماذا لا تقوم بإجهاض طفلك؟
◀ نبحث عن معدل وفيات من الكورونا أعتقد أنه 0.2٪ وهناك بعض التساؤلات حول ما إذا كان يجب اعتبار المرضى الذين يعانون من أمراض مصاحبة حالات الوفاة من الكورونا. متوسط عمر المرضى الذي يقال إنهم يموتون من COVID حوالي 79 إلى 83 عامًا.. 😎
◀ قول “عملنا يعود لعقود”.. لا يعني ذلك أنه آمن، بل يعني أننا لم نحقق نجاحًا منذ عقود 😎
◀ عدد من اللقاحات التي طورتها منظمة Word Health القصد منها العقم عن قصد.
عندما تدخل ويقول طبيبك “هل ترغب في أن تحصل ابنتك عَ Gardasil ” لم يتم إخبارك بأنها قد تصاب بأمراض المناعة الذاتية الرهيبة التي ارتبطت بها بما في ذلك متلازمة التعب المزمن ومتلازمة تسمى PoTS..😎

ما يلي نص تقريبي لمقابلة جون هنري ويستن John-Henry Westen’s المؤسس المشارك في LifeSite مع باميلا أكير Pamela Acker ، باحثة وخبيرة في مجال اللقاحات.
جون-هنري ويستن: مرحبًا بكم في هذه الحلقة من برنامج John-Henry Westen Show ، حيث يسعدني جدًا إستقبال باميلا أكير، وهي باحثة في مجال اللقاحات، وقد نشرت كتابًا جديدًا بعنوان اللقاحات وفق النظرة الكاثوليكية. لذلك أسأل عما تحدث عنه الأسقف أثناسيوس شنايدر Bishop Athanasius Schneider ، بخصوص اللقاح المُلوّث بخلايا جنين مُجهض، سيما لقاحات COVID.. ولنبدأ كما نفعل دائمًا عند إشارة الصليب. بسم الآب والابن والروح القدس آمين…
باميلا أكير Pamela Acker : شكرًا جزيلاً لك ، يسعدني أن أكون هنا.
John-Henry Westen’s) JHW ): بدايةً أخبرينا قليلاً عن نفسك، عن خلفيتك في مجال التطعيمات هذا.
PA: شاءت الظروف أن أكون شاهدة على دراسة انشطة اللقاحات، كنت متحمسة بشأن اللقاحات منذ حوالي 20 عامًا، قبل أن يصبح موضوعًا ساخنًا اليوم لـCOVID. عندما كنت في المدرسة الثانوية كنت شغوفة بدراسة علم الأحياء، ومهتمّة بشكل خاص بدراستها لأنه في ذلك الوقت كان هناك بعض الاعتقاد بأن النباتات يمكن أن تكون معدلة وراثيًا لتوصيل اللقاحات. وفي حينه وجدت أمرين مثيرين للغاية، أحدهما أنه يمكنك أن تأكل شيئًا كون لا أحد يحب وضع الإبر تحت الجلد. والأمر الثاني هو أن ذلك قد يسهل توزيع اللقاحات في دول العالم الثالث، لأنه لا داعي للقلق بشأن التبريد الخاص أو المكونات القابلة للتلف، لأنه يمكنك فقط زراعته في البلدان الأخرى.
بعد ذلك ، حصلت على درجة الماجستير من الجامعة الكاثوليكية الأمريكية في عام 2010 ، 2012 ، كنت هناك بالفعل للحصول على درجة الدكتوراه ، لكنني تركت درجة الماجستير لأن المعمل الذي دخلت فيه، والذي كان يشارك أيضًا في تطوير اللقاحات، كان يعمل على مشروع لقاحات فيروس نقص المناعة البشرية. وكان تمويل المنحة في إطار مؤسسة Bill & Melinda Gates، وقد حصلنا على المرحلة الأولى من المنحة، وكنا مستعدين للتقدم للمرحلة الثانية ومحاولة تحقيق نتائج جيدة كون خطتنا كانت قابلة للاستمرار هناك.
كان هناك اجتماع عمل وكان الجميع جالسًا، قال المشرف الرئيسي، “على الجميع المشاركة في جزءٍ معين بالمشروع” وكان المشروع يتعلق بخلايا “HEK-293“. وهذه النقطة اليوم نسمع بها كمعظم الناس لأنها مرتبطة بلقاحات COVID ، لكن في ذلك الوقت سألت زميلتي عن معنى HEK ، فـأخبرنتني: بأنها “كلية جنينية بشرية”.
أمضيت أسبوعان في البحث عما يعنيه ذلك، وجدت عمل ألفين وونغ Alvin Wong من المركز القومي لأخلاقيات البيولوجيا الكاثوليكية، الذي كتب مقالاً في … أعتقد أنه كان عام 2005 أو 2006 ، بعنوان الأخلاق من HEK-293. ويساعدني عمله كثيرًا في تمييز ما إذا كان بإمكاني المشاركة بالفعل في هذا المشروع أم لا. وعندما عبرت عن مخاوفي لمحققتي الرئيسية، انتهى بي الأمر إلى نهاية مسيرتي المهنية في مختبره.
لذلك، لم أحصل على درجة الدكتوراه، غادرت مع ماجستير. لكن استخدام الخلايا الجنينية المجهضة في اللقاحات هو بالتأكيد مسألة عزيزة على قلبي، وقد أثر ذلك كثيرًا على حياتي حتى اليوم. لكنني أيضًا تمكنت من البقاء في المختبر لمدة 9 أشهر تقريبًا قبل إثارة هذه المشكلة الأخلاقية، لذلك لدي خبرة بحثية مباشرة حول تطوير اللقاح.. وقد مكنني ذلك على ما أعتقد، أن يكون لي صوتٌ فريد في هذه الحجة الآن.
JHW: صحيح، أنتِ مؤهلة بشكل جيّد لمناقشة هذا الموضوع أكثر من غيرك، كونك عملتي داخل المختبر وكذلك على اللقاحات. ولك كتابٌ عن ذلك..
PA: بدأت هذا الكتاب منذ عامين تقريبًا. في إحدى ليالي الشتاء، سقطت وأصبت كاحلي، وبقيت على هذه الحال فترة طويلة.. في حينه مركز كولبي كان ورائي للنظر في مسألة اللقاحات لفترة من الوقت. وعندما كنت على الأريكة دون أن أفعل شيئًا أفضل ، قرأت كل الأشياء التي لا يوجد وقت لقراءتها ، كان ذلك عندما بدأت بالفعل البحث عن هذا الكتاب.
لذلك ، بدأت بالفعل في شهر أبريل من عام 2019 ،قبل أن يكون COVID يمثل مشكلة على الإطلاق ، ومن هنا كان السبب في أن الكتاب كان جيدًا وفي الوقت المناسب.
JHW: هذا حقًا بفضل العناية الإلهية. لذلك ، نحن في وقت “مجنون” تمامًا سيما مع قضية اللقاحات، التي كانت موجودة منذ عقود عديدة حتى الآن، قد اتخذت طابعًا عاجلاً جديدًا تمامًا مع ما يبدو أنه سيتم فرضه على الجميع. على الرغم من أن الجميع تقريبًا يقول “لا ، لا ، لن نجبرها أبدًا”. في الواقع ، لقد تحدثوا بالفعل عن ، “أنت بحاجة إلى التطعيم لأخذ رحلة ، تحتاج إلى التطعيم للذهاب إلى متجر.” نحن نرى بالفعل مع تفويضات القناع وتفويضات التباعد الاجتماعي ، والإغلاق وكل شيء آخر ، أنهم مستعدون حقًا لاتخاذ إجراءات صارمة. لذلك ، في حين أنه قد لا يتم إجبارك على الضغط والتطعيم ، ستصبح حياتك غير قابلة للعيش إذا لم تأخذها.
إذن ، هذا هو حالتنا. الآن ، عندما ننظر إلى أخذ اللقاحات ، بصفتنا أحد الوالدين ، قمنا بتقييم أشياء مثل ، “هل هو ضروري؟ هل هو آمن؟ هل هي فعالة؟ ” لكن أحد الأسئلة أيضًا هو ، “هل هذا أخلاقي؟” ولذا ، أود أن أتحدث معك عن كل هذه النقاط ، فيما يتعلق بلقاحات COVID التي تمت الموافقة عليها الآن ، وماذا يعني أنها ملوثة بالإجهاض؟ لذا ، إذا استطعنا البدء بشكل صحيح بالإجهاض الملوث، لأنني أعتقد أنه بالنسبة لمعظم الناس، فإن أحد العوامل المؤهلة لأخذ لقاح في المقام الأول هو طبيعته الأخلاقية. “هل من الأخلاقي أن تأخذ هذا؟
PA: اللقاحان المعتمدان حاليًا هما لقاح Moderna ولقاح Pfizer ، وكلاهما لقاح mRNA، وبالتالي على المستوى الجزيئي هما متشابهان جدًا. تمّ تصنيع كلا اللقاحين باستخدام تقنية التكنولوجيا الحيوية التي يمكنها تصنيع الأحماض النووية في المختبر. لذلك ، يحاول الكثير من الناس المجادلة بأنهم أخلاقيون لأن mRNA الذي تم تصنيعه لا يلامس أبدًا الخلايا الجنينية. ولكن هذا ليس كل ما في القصة عندما تنظر إلى الطريقة التي تم بها تطوير هذه اللقاحات.
وهكذا ، توثق الأوراق البحثية الأصلية استخدام خلايا HEK-293 في إنتاج هذه اللقاحات. وهكذا ، تم استخدامها بطريقتين مختلفتين. أحدها أن بروتين السنبلة …
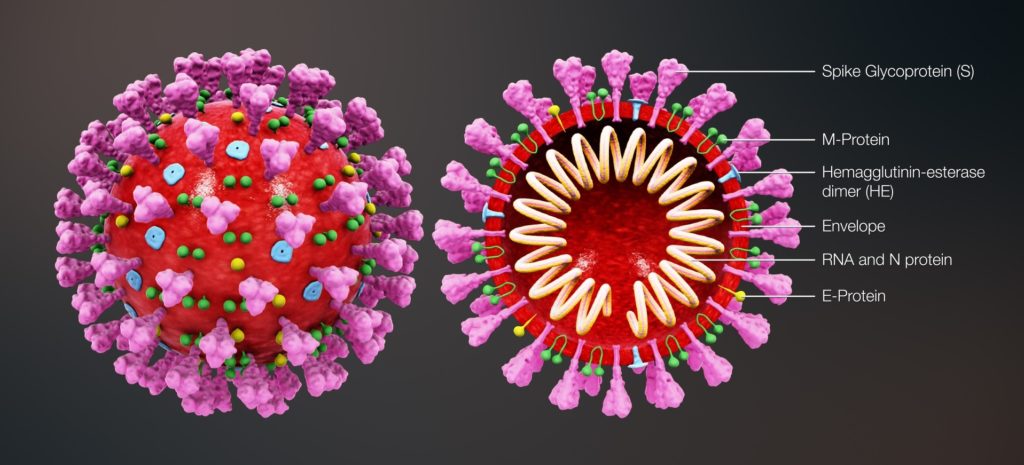
يمكنه فقط القيام بدورة بيولوجية تصادم مدتها ثلاث دقائق. mRNA هو رسول RNA ، وهو الحمض النووي الذي هو نسخة مصنوعة من الحمض النووي الخاص بك ، ثم يتم إرساله إلى الريبوسومات في الخلايا ويتم إنتاج البروتين باستخدام نسخة المرسال هذه. لذا ، ما يفيده اللقاح هو أن يأخذ مرسال الحمض النووي الريبي (messenger RNA) الذي يرمز إلى بروتين سبايك spike لفيروس كورونا وإدخاله في خلاياك حتى تصنع خلاياك البشرية بعد ذلك بروتين سبايك من فيروس كورونا.
والفكرة هي أن هذه ستكون طريقة فعالة جدًا لتطعيمك لأننا وجدنا أنه إذا أخذت بروتين spike وحقنته في الناس ، فإنه يميل إلى التدهور بسرعة كبيرة جدًا للاستجابة المناعية الجيدة. تميل إلى وجود بعض التعقيدات الأخرى التي سأتطرق إليها لاحقًا في المقابلة. لكن الفكرة هي أنه إذا كان جسمك يصنعه بنفسه، فيمكنك أن تتعرض لفترة طويلة بما يكفي لبروتين السنبلة حتى تتمكن من تكوين استجابة مناعية له. لذلك ، هذه هي الطريقة الأساسية التي من المفترض أن يعمل بها.
لذا ، فإن بروتين سبايك في حد ذاته ، على حد تعبير أحد الباحثين ، نوع مرن ، لا يميل إلى الحفاظ على شكله جيدًا. وهكذا ، صمم العلماء وراثيًا بروتينًا شائكًا يحافظ على شكله ، وقد حصل على بعض الطفرات التي تسبب استقراره. وهكذا ، هذا التصميم الأصلي لهذا البروتين … لذلك ، عندما قاموا بتحوره في الأصل … كانوا بحاجة لمعرفة ما إذا كان سيحافظ على شكله بشكل صحيح ، إذا كان هذا سيصحح مشكلة المرونة. لذلك ، أخذوا تلك المعلومات الجينية ، وقاموا بتحويل الخلايا لإنتاج بروتين سبايك حتى يتمكنوا من تنقيته وإلقاء نظرة عليه باستخدام تقنيات لتصور البنية ثلاثية الأبعاد للبروتينات. وقد أجريت تلك التجربة الأصلية في خلايا HEK-293. لذا ، فإن البروتين الشائك الذي تم تطويره في شفرة اللقاحات ، تم تطويره في الأصل بشكل فعال في خلايا الجنين المجهضة.
والطريقة الإضافية التي تم بها استخدام الخلايا الجنينية المجهضة في المشروع هي ، قبل أن يقوموا بحقنه في كائن بشري لمعرفة ما إذا كان بإمكانك الحصول على الخلايا البشرية لصنع بروتين فيروس كورونا ، قد ترغب في اختبار ذلك في ثقافة الخلية ، قد ترغب في اختبار ذلك في المختبر. لأنه أقل تكلفة وخطورة بكثير من اختباره على الإنسان. وبالتالي ، إذا لم تتمكن حتى من الحصول على الخلايا في المختبر لتصنيعها ، فمن المحتمل ألا تتمكن من جعل جسم الإنسان يصنعها. لذا ، فإن الخلايا التي تم اختبار ذلك فيها كانت أيضًا خلايا HEK-293. وقد تم نشر هذا كله في الأدبيات ، وقد قرأت بضع ورقات توثق أن كلا اللقاحين استخدم HEK-293 في اختبارهما.
ويريد الكثير من الناس أن يقولوا ، “حسنًا ، لقد تم ذلك للتو لتطوير اللقاح في البداية ، لذلك الجزء البحثي … لذلك ، لقد كان شيئًا وفعلت شيئًا ما ، إنها ليست مشكلة كبيرة.” ولكن مؤخرًا ، نشرت Stacy Trasancos مقالًا متاحًا على موقع Children of God for Life على الويب ، وأشارت إلى … وبصفتي باحثة يمكنني أن أؤكد أنها على حق تمامًا ، أن هذه الأشياء أيضًا يجب أن تخضع لاختبار مراقبة الجودة. لذلك ، في كل مرة أقوم فيها بعمل دفعة أخرى من الrna الحمض النووي ، والتي يتم تصنيعها باستخدام تقنية معملية ، فأنا بحاجة إلى الاختبار والتأكد من أنها لا تزال قابلة للتطبيق ، وهذا أمر شائع إلى حد ما ، للحصول على مراقبة الجودة مثل ذلك في المختبر.
لذلك ، قد يكون الاختبار مع هذه الخلايا الجنينية المجهضة مستمرًا بالفعل في إنتاج هذه اللقاحات. لأنه بشكل عام ، عندما ترفع إنتاج اللقاح إلى ما بعد البحث والتطوير ، فإنك ستستخدم نفس إجراءات الاختبار لاختبار النطاق الذي تستخدمه لاختبار الدفعة الأصغر ، ما لم يكن ذلك لسبب ما غير ممكن. لكن هذه طريقة مجدية للغاية لاختبار ذلك لهؤلاء الباحثين. إنها ليست طريقة أخلاقية ، لكنها مجدية للغاية لأن هذه الخلايا قد تم تحسينها للاستخدام في المختبر. وهم موجودون في كل مكان تقريبًا في أبحاث زراعة الأنسجة، للأسف هناك الكثير من المختبرات حول العالم التي تستخدم خلايا HEK-293 هذه. وهناك منتجات محددة تم تحسينها بشكل أساسي لتتمتع بظروف نمو مثالية. لذلك ، هناك صناعة كاملة تعتمد على هذه الخلايا الجنينية المجهضة في أبحاث العلوم الأساسية التي أعتقد أن الناس ليسوا على دراية بها.
JHW: لذا ، فقط للتوضيح ، لقاحا COVID-19 ، كلا من Pfizer و Moderna ، لم يتم تطويرهما فقط في بروتين سبايك مع HEK-293 ، خط الخلايا الجنينية المجهضة ، ولكن أيضًا في اختباراتهم الأولية. والآن تخبرنا ، على الأقل من هذه المقالة من Stacy Trasancos ، في الاختبار المستمر حاليًا للدفعات الجديدة.
PA: نعم. بقدر ما أعرف ، هناك اختبار مستمر حاليًا للدفعات. لم يتم نشر ذلك في الأدبيات في حد ذاتها ، لأنه لم يتم نشر أي بيانات بعد التجارب السريرية الأولية ، ولكن هناك سببًا جوهريًا للاعتقاد بأن هذا يحدث.
JHW: دعنا نتوقف عند هذا الحد، لأنني أعتقد أن على الناس أن يفهموا شيئًا عن HEK-293 و PER.C6 ومجموعة من سلالات الخلايا الجنينية المجهضة الأخرى الموجودة هنا . وهذا يتعلق بتطورهم الأولي على أي حال ، لأنني أعتقد أن الكثير من الناس لديهم انطباع بأن … ليس الآن ، لأنك قلت بالفعل ما قلته فيما يتعلق باستخدام HEK-293. لكن ، أعتقد أن الكثير من الناس تحت الانطباع ، “حسنًا ، كان هذا طفلًا واحدًا قُتل في السبعينيات وهو بعيد جدًا عن ذلك التاريخ الآن ، وهذا شيء مقبول علينا فقط التعايش معه لأنه ينقذ الكثير من الأرواح “. فما هو HEK-293 بالضبط؟ وهل كان مجرد طفل واحد هو المسؤول عن ذلك ، وماذا عن سلالات الخلايا الجنينية الأخرى؟
PA: هناك عدد من سلالات الخلايا الجنينية موجودة الآن ، وسأقرأ القليل منها من “أطفال الله من أجل الحياة”. هناك WI-38 و MRC-5 و HEK-293 و PER.C6 ، وهناك واحد آخر تم تطويره في عام 2015 ولا يتم استخدامه حاليًا في أي لقاحات، ولكن يمكن استخدامه في لقاحات ويستخدم في علاجات أخرى. لذلك ، هناك عدد من خطوط الخلايا هذه التي يتم استخدامها حاليًا لتطوير مجموعة متنوعة من العلاجات ، كل شيء من اللقاحات إلى علاجات التليف الكيسي.
معظم الناس ، كما تقول ، يرفضونها بيد تلوح لهم ويقولون ، “حسنًا ، لقد مات طفل واحد ، لا يمكننا العودة والتراجع عنه ، وربما نحصل على شيء جيد منه الآن.” وهذا بالطبع ينتهك مبدأ الصالح المتكامل ، وحقيقة أنك ببساطة لا تستطيع استخدام الغايات لتبرير الوسيلة. لكنني لست عالم لاهوت أخلاقي ، لذلك سألتزم بالعلم.
بالنسبة لـ HEK-293 ، كان ذلك… أحد الأشياء التي رأيتها ظهرت عدة مرات في المقالات التي نظرت إليها حول الاعتبارات الأخلاقية التي ينطوي عليها الأمر ، وهو أن الناس يقولون ، “حسنًا ، لم يكن هناك توثيق أن ذلك كان إجهاضًا اختياريًا ، لذلك يمكن أن يكون إجهاضًا تلقائيًا “. وهذا مخادع بعض الشيء أو جاهل من جانب هؤلاء المؤلفين ، لأنه من أجل إنتاج خط خلوي قابل للحياة ، هناك عدد من الأشياء التي تدخل في ذلك ، وهو أمر صعب للغاية.
وهكذا ، كنت أقوم ببعض الأبحاث تحديدًا على HEK-293 للتحضير لهذه المقابلة ، ونظام الأرقام المتضمن هناك … يرمز HEK إلى Human Embryonic Kidney ، ولكن 293 تعني هذه التجربة 293 التي قام بها هذا الباحث تحديدًا تطوير خطوط الخلية. وهذا لا يعني أنه كان هناك 293 عملية إجهاض، ولكن بالنسبة لـ 293 تجربة ، فأنت بحاجة إلى أكثر من إجهاض واحد. ونحن نتحدث على الأرجح عن مئات من عمليات الإجهاض. وقد تم ذلك بالتعاون مع بعض المستشفيات. وكانت هناك مجموعة في السويد شاركت في تطوير خط خلية WI-38 ، لذلك كان هناك خط خلوي مختلف ، لكنهم كانوا يقومون بشكل روتيني بإجهاض الأطفال لاستخدامهم في محاولة تطوير سلالات الخلايا الجنينية.
لذا ، عادة ما يكون لدى الناس في هذه المرحلة سؤال ، “لكن لماذا؟ لماذا خط الخلايا الجنينية؟ “ وعندما تحاول إنماء الخلايا في مزرعة في المختبر ، فإنها تمر بعملية تسمى الخلود ، لتطوير خط خلوي. والناس يخلطون في ذلك نوعًا ما ، لأنه يبدو أنهم يعيشون إلى الأبد ، مع التفكير في أنه يمكنك جعل هذه الخلايا تعيش إلى الأبد في المختبر. لا يمكنك. يمكنك جعلهم يعيشون لفترة أطول بكثير من زراعة الخلايا الأولية، إذا كنت ستأخذ شيئًا من ذراعي وتنمو في طبق بتري ، فسيبقى على قيد الحياة لبضعة أقسام فرعية ، ولكن ليس كثيرًا. ولكن ، إذا أدخلت بعض الطفرات فيه ، فيمكنه البقاء لفترة أطول. وهذا ما يكون لديك عندما يكون لديك خط خلوي خالٍ ، يكون لديك شيء تم تحوره عادةً بجينات الورم الفيروسية. وهذه هي الجينات التي تعزز السرطان في الواقع ، لذا ضع إشارة مرجعية هناك أيضًا لأن هذا مهم لشيء نأمل أن نناقشه لاحقًا في المقابلة ، حول بعض مخاطر استخدام … فقط المخاطر البيولوجية ، ناهيك عن الأخطار الأخلاقية لاستخدام لقاحات الخلايا الجنينية المجهضة.
غالبًا ما تُعطى سلالات الخلايا الخالدة جينات معززة للسرطان والتي تعطل وظيفة الجينات الكابتة للسرطان أو الجينات الكابتة للورم. وهكذا ، يمكن أن تنمو ، ليس إلى أجل غير مسمى تمامًا ، ولكن لأجيال عديدة في المختبر. إذا بدأت بالخلايا البالغة ، فسيكون لديك عمر افتراضي أقصر ، لأن الخلايا البالغة قد خضعت بالفعل لعدد معين من انقسامات الخلايا ، وبالتالي فإن هذا النوع من التهم في العدد الإجمالي الذي يمكن أن تخضع له بالفعل. وبالتالي ، إذا كنت تستخدم الخلايا البالغة في المختبر ، فسيكون لديك عمر أقصر لخط الخلايا لديك ، وسيتعين عليك تطوير خط خلوي جديد في وقت أقرب ، وهو ليس مجديًا تجاريًا. إذا بدأت بالخلايا الجنينية، فسيكون لديك أقصى عمر متاح لخط خليتك ، ولذا أعتقد أنه ربما كان أحد الأشياء التي تم استخدامها لتبرير استخدام هذه الخلايا الجنينية المجهضة كبداية.
وبعد ذلك ، هناك سؤال آخر يطرحه الناس وهو ، “حسنًا ، لماذا لا يكون HEK-293 مجرد إجهاض تلقائي؟ لماذا لا يكون مجرد إجهاض؟ لأن المستشفى فقدت الوثائق المتعلقة بهذا الطفل بالذات والتي تم استخدامها لتطوير الخط الخلوي ، ولذا فإننا لا نعرف حقًا ما إذا كان إجهاض اختياري أم إجهاض تلقائي”. حسنًا ، لدينا جميع الأسباب في العالم للاعتقاد بأنه كان في الواقع إجهاضًا اختياريًا تم إجراؤه عن قصد ، لأن الباحثين الذين شاركوا في هذا النوع من الأشياء سجلوا في الأساس قولهم ، “يجب أن تحصل على ذلك الأنسجة في غضون حوالي خمس دقائق من الإجهاض لكي تكون قابلة للحياة على النحو الأمثل ، وإذا انتظرت لمدة ساعة ، فهذا عديم الفائدة “.
لذلك ، إذا كنا نتحدث عن إجهاض تلقائي ، فإن هذا الطفل يموت قبل وقت طويل من إزالة أنسجة الجنين من جسم الأم. هذا الإجهاض التلقائي أو هذا الإجهاض لن يكون قابلاً للتطبيق لبدء خط خلوي على الإطلاق ، لن يكون هناك طريقة يمكنك من خلالها الحصول على خط خلوي حي من الأنسجة الميتة. لذلك ، كان لابد أن يكون هذا طفلًا تم إجهاضه وكانوا يعرفون أن هذا النسيج سيُستخدم في البحث حتى يتمكنوا من الوصول إلى هناك في غضون خمس دقائق إلى نافذة ساعة ، ويفضل أن يكون ذلك خلال الدقائق الخمس الأولى ، من أجل الحصول على هذا النسيج المحفوظ.
JHW: هذا يذهب مباشرة إلى فضيحة جزء الطفل التي نتعامل معها الآن ، حيث يسأل باحثو الجامعة الأم أولاً ، “نحن نبحث عن كلية أو ذراع أو أي شيء لتجربته ، لذلك عندما تقوم بذلك” سوف تقومين بالإجهاض على أي حال ، هل يمكنك القيام بذلك؟ ” وفي بعض الأحيان اطلب منهم الانتظار لفترة أطول حتى يتم تطويره بشكل أكبر ، بحيث يكون لديهم عينة أفضل. مقزز تماما. لذا ، استمر هذا حتى مع اللقاحات ، أن هذا لم يكن إجهاضًا مخططًا فحسب ، بل كان إجهاضًا مخططًا واستخراج أنسجة جنينية [00:20:31] تُستخدم في غضون خمس دقائق من الإجهاض. لذا ، فإن الهراء حول كونه إجهاضًا واضحًا تمامًا.
PA: إنه أسوأ من ذلك لأن… وهذا هو المكان الذي أصدر فيه تحذيرًا دائمًا ، إذا كان هناك أي آذان صغيرة تستمع إلي وأنا أتحدث على التسجيل ، لأنه يحتوي على رسوم بيانية أكثر بكثير مما لدي وصف للتو. لأنه ، في كثير من الحالات ، الأطفال … لأن ذلك يتم عن قصد لأغراض بحثية ، لذا فإنهم في الواقع سيولدون هؤلاء الأطفال بعملية قيصرية ، في بعض الحالات يظل الأطفال على قيد الحياة عندما يبدأ الباحثون في استخراج الأنسجة. لدرجة أن قلبهم لا يزال ينبض ، ولا يتم إعطاؤهم أي مخدر بشكل عام لأن ذلك من شأنه أن يعطل الخلايا التي يحاول الباحثون استخلاصها. لذا فهم يزيلون هذا النسيج عندما يكون الطفل على قيد الحياة ، وبكميات كبيرة من الألم ، وهذا يجعله أكثر سادية.
وقد ألقى راعي أبرشيتي مؤخرًا خطبة شبيهة بما اعتاد الأزتيك القيام به، عندما كانوا يكرسون معابدهم ، كانوا ينتزعون حرفيًا القلوب النابضة للضحايا الذين كانوا يذبحون فوق المعابد ، ثم يلقيون بها. جثث أسفل الجانب. هذا هو بالضبط نفس الشيء الذي يفعله هؤلاء الباحثون.
JHW: أجل. وقد ذكرت ، أننا نخرج الكلى الجنينية البشرية ، HEK ، لذا فهي الكلية التي يجب عليهم الوصول إليها. لذا ، فهم يقطعون هؤلاء الأطفال الأحياء ، وقد تم ولادتهم للتو بعملية قيصرية … نعم ، وربما يكونون أصغر من أن يعيشوا خارج الرحم بمفردهم على الفور ، لكنهم ما زالوا أحياء بدرجة كافية ، ونحن نعلم بالفعل أنهم أشعر بالألم. وبعد ذلك ، يفتحونها لأخذ … يجب أن يكون معروفا. لأنني أعتقد أن الكثير من تحديد أخلاق هذه الأشياء ، حتى الأخلاق مفصولة بسنوات ، وبالتالي فهي اتصالات بعيدة ، كما يسمونها ، لا أعتقد أنهم أخذوا في الاعتبار ما هو هذا في الواقع. هذا هو السبب في أن العلم الذي تقدمه هنا مهم للغاية ، لأن الأشخاص الذين اتخذوا هذه القرارات … ونعلم جميعًا …
واسمحوا لي فقط أن أوضح ، أنه في عام 2005 ، خرج الفاتيكان أولاً ، من خلال الأكاديمية البابوية للحياة ، بوثيقة تقول أن استخدام مثل هذه اللقاحات ، إذا لم يكن هناك أي لقاحات أخرى متاحة ، وإذا كان اعتراضك على إجراء كيف تم تطويره معروف ، وإذا لزم الأمر ، فهو مقبول أخلاقيا إلى حد ما. ولكن ، حتى في ذلك الوقت … كان هذا في عام 2005 ثم تم ختمه بالمطاط ، على ما أعتقد ، في عام 2008 مع CDF. لكني لا أعرف أن هذه الحقائق كانت معروفة في ذلك الوقت.
PA: بالتأكيد. لذلك ، بما أنك أشرت إلى الوثيقة من قبل الأكاديمية البابوية للحياة ، فإنني أعالج ذلك في الكتاب الذي كتبته عن التطعيم ، وهناك بعض المشاكل الحقيقية مع العلم الذي تم تقديمه للأشخاص الذين كانوا يتخذون تلك القرارات. لأن إحدى أقوى النقاط التي استخدموها لتبرير الموقف الذي يتخذونه ، من حيث “يمكن السماح بهذه اللقاحات إذا كان الوضع خطيرًا بدرجة كافية” ، هي حوادث متلازمة الحصبة الألمانية الخلقية.
الآن ، متلازمة الحصبة الألمانية الخلقية، هذا عندما يصاب الطفل بالحصبة الألمانية من أمه في الرحم في الأشهر الثلاثة الأولى ، ويمكن أن يؤدي إلى العمى ، والصمم ، والبطء العقلي ، وحتى ولادة جنين ميت ، لذلك هو مرض خطير. الآن ، الحصبة الألمانية نفسها ليست مرضًا خطيرًا بشكل خاص ، خاصة إذا تم التقاطها في مرحلة الطفولة، فمعظم الناس لن تظهر عليهم أعراض. وأعتقد أن أكثر من نصف الحالات ، لا يقوم أحد برحلة إلى الطبيب لأنه لا يوجد شيء ملحوظ أو يحدث. ولذا ، يعد هذا مرضًا خفيفًا جدًا عند الأطفال ، وهو في الحقيقة مشكلة فقط لدى النساء الحوامل اللائي يصبن به خلال الأشهر الثلاثة الأولى من الحمل.
وكان الفكر هو ، “حسنًا ، التطعيم ضد الحصبة الألمانية سيحمي هؤلاء النساء الحوامل ، وبالتالي فهو مبرر أخلاقياً.” ولكن ، في موقف ما … من المحتمل أن يكون مشابهًا جدًا للموقف مع COVID ، عندما تنظر إلى الأرقام الفعلية ليس هذا هو الحال. لأنه قبل إدخال لقاح الحصبة الألمانية ، كان هناك ما يقرب من 80٪ من مناعة القطيع في السكان ضد الحصبة الألمانية. و 80٪ مناعة القطيع هي العتبة التي لا ينتشر عندها المرض بشكل جيد. من الواضح أنه لا يزال ينتشر ، وسيظل الناس مصابين بالحصبة الألمانية ، لكنه لا ينتشر بين السكان كالنار في الهشيم ويعرض الكثير من الناس للخطر.
لذلك ، بعد استخدام لقاح الحصبة الألمانية ، لدينا الآن ما يقرب من 80 إلى 85٪ مناعة للقطيع. وهكذا ، قد تقول ، “حسنًا ، هذا أفضل قليلاً ، لذا ربما كان الأمر يستحق ذلك”. ولكن في السنوات العشر الأولى بعد تقديم هذا اللقاح ، لم يكن هناك انخفاض في حالات متلازمة الحصبة الألمانية الخلقية. وفي الواقع ، في السنوات القليلة الأولى بعد تقديمه ، كان هناك ارتفاع في حالات متلازمة الحصبة الألمانية الخلقية ، فقد ارتفعوا. ولم يبدأوا في الانخفاض حتى أصبح الإجهاض قانونيًا. (للتخفيف من نسبة أرقام الوفيات) وهناك حالة جيدة جدًا يمكن إثبات أن الانخفاض في متلازمة الحصبة الألمانية الخلقية كان بسبب إبلاغ أمهاتهم ، “لديك الحصبة الألمانية ، من المحتمل أن يصاب طفلك بمتلازمة الحصبة الألمانية الخلقية ، فلماذا لا تقوم بإجهاضها فقط؟ حاول مرة أخري.” ربما يرجع الانخفاض الذي رأيناه في هذا المرض إلى عمليات الإجهاض الاختيارية أكثر منه بسبب إدخال اللقاح.
لذلك ، لدينا الآن هذا اللقاح الذي لدينا، على ما أعتقد، في جميع أنحاء العالم. يوجد 70٪ من الإقبال على لقاح الحصبة الألمانية، وهي الطريقة الوحيدة للتطعيم ضد الحصبة الألمانية. اعتدت أن تكون قادرًا على الحصول على اللقاح بشكل منفصل، لكن شركة Merck جمعتهم جميعًا معًا في التسعينيات بعد ذعر Wakefield، والذي من المحتمل أن يشير إلى أن MMR كان مرتبطًا بتطور التوحد. وهكذا ، توقفت شركة Merck للتو عن إنتاج اللقاحات المنفصلة، ولا يمكنك الحصول عليها الآن إلا كقاح ثلاثي التكافؤ ضد الحصبة والنكاف والحصبة الألمانية. مما يعني أنه لا يمكن أخلاقياً أن يتم تطعيمك ضد أي من هذه الأشياء لأن اللقاح يتم إنتاجه في خلايا جنينية مجهضة. لقد تم إنتاجه في خط خلية WI-38 ، وقد استغرق ذلك الخط الخلوي ، أعتقد أنه كان 32 عملية إجهاض قبل أن يصلوا إلى خط الخلية هذا. الرقم 38 ، مرة أخرى ، هو عدد التجارب التي تم إجراؤها بالفعل ، وأعتقد أنه كان 32 طفلاً.
ثم الفيروس المستخدم في لقاح الحصبة ، فيروس الحصبة الموهن ، بدلاً من مجرد مسح حلق طفل مريض كما فعلوا في اليابان ، شجع الباحثون الأمريكيون النساء اللائي تعرضن للحصبة الألمانية في الأشهر الثلاثة الأولى من الحمل على الإجهاض الاختياري. الأطفال. قاموا بتشريح 27 جنينًا قبل أن يصابوا بالفيروس المستخدم حاليًا في لقاح الحصبة الألمانية ، واستمروا في 40 عملية إجهاض اختيارية أخرى ، وعزلوا عددًا من السلالات الفيروسية المختلفة التي لم يتم استخدامها في النهاية في اللقاح. ولكن ، إذا جمعت كل ذلك معًا ، فسوف ينتهي بك الأمر مع ما يقرب من 99 عملية إجهاض من أجل لقاح الحصبة الألمانية فقط.
مع الأخذ في الاعتبار أن كل هذه الحالات ربما تتم في نفس الظروف المروعة التي وصفناها للتو، وفي بعض الحالات حيث وُلد الأطفال … تمت إزالة الكيس الأمنيوسي بالكامل من الأم وتم تشريح هؤلاء الأطفال في ذلك الوقت و هناك. وبعض الحالات كانوا عالقين في الثلاجة للحفاظ عليهم قليلاً حتى يمكن تشريحهم بعد ذلك بقليل، فوحشية ذلك والرعب الناتج عن ذلك ليس شيئًا يجب أن نتستر عليه. ومع ذلك ، فإن والدك الكاثوليكي العادي الذي يذهب إلى مكتب الأطباء ويسأل ، “هل تريد MMR؟” لا يعرف حتى كيف تم تطوير هذا..
وهكذا، عندما كان الأسقف شنايدر يتحدث معك في المقابلة التي أجراها معك حول التواطؤ الأخلاقي الذي يُطلب من هذا النطاق الكبير من الناس قبول هذا فقط … هذا ليس شيئًا جديدًا تمامًا مع ظهور COVID، هناك لقد كانت بالفعل نجاحات كبيرة، كما أعتقد، فيما يتعلق بجعل الناس يلائمون الشر لاستخدام شيء له أصل شرير حقًا لمصلحتهم، على الرغم من أنهم لا يتعاونون حقًا في جلب الشر بحد ذاته. وهذا لا يدخل في حقيقة أن الاستمرار في القيام بذلك يغذي السوق لخطوط خلايا إضافية ومنتجات جنينية تم إجهاض إضافية ولقاحات إضافية تُصنع في خلايا جنينية مجهضة. لأنه إذا كنا قد رفضنا لقاح MMR، فلن يكون لدينا لقاحات COVID المصنوعة من الخلايا الجنينية المجهضة. هذا لم يكن ليحدث..
JHW: لدي الكثير من الأسئلة لك ولا أعرف من أين أبدأ. دعني أذهب ، أولاً وقبل كل شيء ، للوصول إلى ما قلته بالفعل. ما الخطأ الذي ارتكبته PAV بالتحديد عندما نظروا إلى العلم ، وماذا كانوا ينقصون؟
PA: لذلك ، كانوا يفتقرون إلى فهم ما إذا كان اللقاح وقائيًا أم لا. لذلك ، فإن اللقاحات بشكل عام لها تأثير وقائي متواضع ضد المرض الذي تحاول الوقاية منه، ولكن تطبيق اللقاح لا يؤثر بالضرورة بشكل كبير على مناعة القطيع التي قد تكون موجودة بالفعل في السكان. وفي الواقع ، مثال جدري الماء هو مثال رائع على مدى كارثة إدخال لقاح يمكن أن يكون في الواقع لمناعة القطيع. لأن ما قمنا به من خلال تطعيم الجميع ضد جدري الماء الآن هو القضاء بشكل فعال على دورة التعزيز الطبيعية.
لذلك ، تعرض والداي لمرض جدري الماء مرة أخرى عندما كنت طفلاً وأصبت بالفيروس، وبالتالي تم إعطاء جهاز المناعة لديهم معززًا طبيعيًا ليقولوا، “ أن فيروس جدري الماء. لماذا لا تقوي استجابتك المناعية قليلاً حتى لا تصاب بِ shingles في غضون سنوات قليلة؟ ” لأنه ناتج عن نفس الفيروس ، وبمجرد إصابتك بالفيروس ، فإنه ينتشر في الخلايا العصبية ، وبالتالي إذا كنت مصابًا بالجدري المائي ، فيمكنك الإصابة بالهربس النطاقي. لكنك لا تميل إلى تطويره إلا بعد فترة طويلة في الحياة بسبب عملية التعزيز الطبيعية هذه. حسنًا ، لقد قضينا على هذا الأمر في السكان الآن ، لذا فقد دفعنا بشكل أساسي متوسط عمر القوباء المنطقية إلى مستوى أدنى ، لذلك نشهد المزيد من حوادث الهربس النطاقي ، ونشاهدها في الشباب. ونحن نراه حتى في الشباب الذين تم تطعيمهم ضد جدري الماء. لأن الفيروس الحي الموهن المستخدم في اللقاح ينتشر أيضًا في الخلايا العصبية ويمكن أن يعود لاحقًا على شكل الهربس النطاقي نفسه.
لذا ، فإن أحد الأشياء التي كانت مفقودة من الأكاديمية البابوية للحياة ، في تصميمهم هنا ، هو أنه لا يمكنك أن تقول فقط ، “اللقاحات تنقذ الأرواح ، وبالتالي فإن هذا اللقاح فكرة رائعة.” عليك أن تنظر إلى اللقاحات على أساس كل حالة على حدة ومعرفة ما إذا كان لها ما يبررها. وتلك التي تستخدم الخلايا الجنينية المجهضة ، بشكل عام ، ليست كذلك ، فهي ليست حقًا لقاحات منقذة للحياة ، وبالتالي ، ليس لديك أمر خطير حقًا. لأنه ، من أجل المشاركة في شر بعيدًا بطريقة مشروعة … وكما قدم الأسقف شنايدر حجة رائعة ، فإننا نوعا ما نلوث المياه بالقول إننا نشارك عن بعد في الشر لأن شر الإجهاض شديد للغاية. ولكن حتى لو كان الأمر كذلك ، فإن الأصل خطير للغاية، يجب أن يكون لديك سبب خطير للغاية حتى تجعله مشروعًا بالفعل. وهكذا ، لم ينظروا إلى العلم بما يكفي ليروا أن السبب لم يكن متناسبًا.
وأعتقد أن الشيء نفسه ينطبق على لقاحات COVID ، فالسبب ببساطة غير متناسب. نحن نبحث عن معدل وفيات من فيروس كورونا ، أعتقد أنه 0.2٪ ومتوسط عمر وفاة مريض تم ترميزه على أنه توفي بسبب COVID … لأن هناك بعض التساؤلات حول ما إذا كان يجب اعتبار المرضى الذين يعانون من أمراض مصاحبة حالات الوفاة من مرض فيروس كورونا. يبلغ متوسط عمر هؤلاء المرضى الذين يقال إنهم يموتون من COVID حوالي 79 إلى 83 عامًا ، ومتوسط العمر المتوقع في الولايات المتحدة حوالي 78.7 عامًا. لذلك من الناحية الفنية ، فإن متوسط عمر وفاة COVID أعلى من متوسط العمر المتوقع في الولايات المتحدة…
JHW: يعتقد الكثير من الناس أنه عندما يأخذون لقاحًا ، “لا يوجد شيء حقيقي للأطفال الذين تم إجهاضهم ، لا شيء حقًا … تم اختباره عليه ، وهو بعيد جدًا ، لا يوجد شيء هناك حقًا. إذا كان هناك شيء متصل بهذا القدر عن بعد فهو مثل جزء من المليار من الجسيم في اللقاح الكامل الذي تحصل عليه “. تحدث عن ذلك، إذا كنت تريد ذلك.
PA: مع لقاحي Moderna و Pfizer ، لا توجد أي مادة جنينية تم إجهاضها متبقية في اللقاحات لأنها لم يتم استنباتها أو إنتاجها مباشرة في الخلايا الجنينية المجهضة. ولكن مع لقاح AstraZeneca ولقاح Johnson & Johnson ضد COVID ، بالإضافة إلى لقاح الحصبة الألمانية ولقاح جدري الماء ، هناك بقايا من هذه الخلايا الجنينية المجهضة التي ينتهي بها المطاف في اللقاحات نفسها. لذا ، عندما تحصل على هذا اللقاح ، فأنت في الواقع تحقن أجزاء من هذا الشخص الذي قُتل في جسمك. وهذه القطع تميل إلى أن تكون بقايا الحمض النووي وبعض حطام البروتين.
لكن الحمض النووي مثير للقلق بشكل خاص ، لأن الدكتورة تيريزا ديشر Dr. Theresa Deisher من شركة Sound Choice Pharmaceuticals ، والتي أعتقد أنها ظهرت إلى الوجود في أوائل القرن الحادي والعشرين. كانوا يعملون أيضًا على حل هذه المشكلة باللقاحات الأخلاقية وتوافر اللقاحات الأخلاقية. لديها بعض الأعمال الهائلة ، وقد لخصت الكثير منها في حديث على YouTube ، حيث نظرت في العلاقة بين زيادة استخدام اللقاحات المشتقة من الخلايا الجنينية المجهضة ، والتي تتوافق مع زيادة معدلات التوحد في البلدان التي نظرت إليها.. وقد حدث هذا في بعض البلدان في أوروبا وكذلك في الولايات المتحدة. وقد رأت أن هناك استجابة تعتمد على الجرعة ، لذا فكلما زاد عدد لقاحات الخلايا الجنينية المجهضة التي نستخدمها ، تزداد حالات التوحد.
لذلك ، قالت ، “دعونا نلقي نظرة على ذلك ، دعونا نرى ما إذا كانت هناك أي آلية معقولة بيولوجيًا لذلك.” ولذا فقد أوضحت أنه عندما تضع ملوثات الحمض النووي للجنين المجهض في كائن بشري حي ، يمكن أن يحدث شيء ما … وهذا يحدث في المختبر ، في ثقافة الخلايا في المختبر ، والتي تسمى إعادة التركيب المتماثل ، حيث يتم حقن الحمض النووي في يمكن للفرد أن يصطف نوعًا ما مع الحمض النووي الذي يتوافق معه في تلك الخلايا الفردية ، ومن ثم هناك بعض الإنزيمات التي يمكن أن تأتي معًا ويمكنهم تبديل هاتين القطعتين. لذلك ، ينتهي بك الأمر بفقدان الحمض النووي الفعلي ودمج الحمض النووي من الخلايا الجنينية المجهضة في خلاياك.
وكانت تقول كيف يمكن لهذا أن يفسر لماذا في بعض الأفراد المصابين بالتوحد … على الرغم من أنه ليس كل ذلك لأن التوحد هو مشكلة متعددة الأوجه للغاية ولا توجد إجابة واحدة صارمة عن سبب تطوره لدى بعض الأفراد وليس لدى آخرين. لكن ، في بعض الأفراد ، ترى المئات مما يسمى طفرات دي Novo Mutations ، لذا فهذه طفرات ظهرت من بدون سبب، ولم يكن لدى والديهم ، ولا يجب أن ترى مئات الطفرات في طفل من جيل واحد فقط . ربما لا يزال هذا الطفل صغيرًا جدًا أيضًا ، ربما لا يمكن أن يكون قد تراكمت كل هذه الطفرات. حسنًا ، يمكنهم ذلك ، إذا كان هذا الحمض النووي المتحور … لأنه إذا كنت تتذكر من البداية في بداية الحديث ، فقد تحدثنا عن كيف أنه من أجل تخليد خطوط الخلايا ، فإننا نلصق الجينات الورمية الفيروسية فيها ، وهذه الجينات تعزز السرطان ، وهذه الطفرات فيها من أجل الحفاظ على نموها في زراعة الخلايا، إلى أجل غير مسمى. لقد تحور الحمض النووي في هذه الخلايا بالتأكيد ، لذلك قد يكون هذا مصدر الطفرات التي نراها في بعض هؤلاء الأطفال الذين يصابون بالتوحد.
لذلك ، هذه إحدى الآليات المحتملة لسبب رؤيتنا لذلك. وهو ليس خارج نطاق الاحتمال بيولوجيًا ، ولكنه أيضًا يكون منطقيًا إذا فكرت فيه ، فقط من القانون الطبيعي. إذا كنت ستفعل شيئًا شنيعًا مثل حقن بقايا شخص قُتل في نفسك ، فستكون هناك نتيجة طبيعية لذلك. لا يمكنك فعل ذلك فقط وليس لديك أي آثار سلبية ، إذا كان ذلك منطقيًا.
JHW: حسنًا ، نحن بالتأكيد في الجزء المتعلق بالسلامة من المناقشة. وأود حقًا الخوض في ذلك ، خاصة فيما يتعلق بما نراه الآن من بعض الأشخاص الذين أخذوا بالفعل لقاحات COVID ، إما سلالتهم. لقد رأينا ممرضة تخرج لتقول أن أحد جانبي وجهها … كانت تعاني من شلل بيل ، ويبدو أنها مشلولة في جانب واحد من وجهها. كان لدينا ممرضة واحدة تناولتها في وقت مبكر وفقدت الوعي. كان لدينا طبيب آخر أخذه ويبدو أنه مات. هل يمكن أن تكون مرتبطة باللقاح؟ وما هي بعض مخاوف السلامة الأخرى المتعلقة بلقاحات COVID ، تلك التي تمت الموافقة عليها وتلك التي تنتظر الموافقة الآن؟
PA: تتمثل إحدى مخاوف السلامة الرئيسية في أي لقاح من لقاحات COVID قيد التطوير في أن معظمها من ما يسمى تقنيات Nextgen technologies . هذه أشياء لم يتم إجراؤها في اللقاحات في الماضي ، لذا فنحن لا نعرف حقًا كيف لقاحات mRNA ، ولا نعرف أي نوع من الآثار الصحية طويلة الأمد التي ستحدث. نحن لا نعرف حقًا ما هي الآثار التي ستحدث في الجسم حتى على المدى القصير. لأنه ، أحد المخاوف التي لدي للتو من التفكير في لقاحات الهندسة الوراثية ، يعود إلى أواخر التسعينيات عندما كانوا يحاولون جعل هذه الثمار تنتج مستضدات اللقاح وتنتجها بجرعات مناسبة. عندما تقوم بإجراء عدوى وراثية للنبات وتحاول جعله ينتج ، على سبيل المثال مستضدات الجدري ، كانت لديهم مشكلة كبيرة في توحيد الجرعة ، وهذا هو سبب إلغاء هذه التقنية في النهاية. لأنهم ببساطة لا يستطيعون قول ذلك ، “إذا أكلت موزة واحدة ، فستحصل على هذا القدر من مستضد الجدري.” لأن كل أنواع الموز كانت مختلفة. وربما يكون الموز مثالًا سيئًا لأن الموز متعدد الصيغ الصبغية وبالتالي هناك بعض المشكلات الوراثية الأخرى التي تحدث هناك. لكن لم يكن أي من النباتات التي اختبروها قادرًا على توحيد المقاييس من حيث الجرعة.
لذلك ، عندما تقوم بإدخال مادة وراثية أجنبية … وهذا صحيح تمامًا مع المختبر أيضًا. ولكن عندما تقوم بإدخال مادة وراثية غريبة في كائن حي ، لا يمكنك التحكم بالضبط في كمية البروتين التي سينتجها هذا الكائن بناءً على كمية الحمض النووي التي تعطيها إياه. ويمكنك نوعًا من تخمين النطاق ، ولكن عندما تتعامل مع شيء مثل بروتين السارس SARS-CoV-2 الشائك … ونحن نعلم أن إحدى الطرق التي يتم بها التوسط في علم الأمراض والأشخاص الذين يمرضون حقًا ، هو من خلال هذه الاستجابة المناعية المفرطة النشاط. تحصل على عاصفة السيتوكين ، وتحصل على كل شيء مضخمًا لدرجة أن نظام المناعة لديك هو في الواقع ما يقتل جسمك. سنقوم بعد ذلك بأخذ المعلومات الجينية ، وإلصاقها بجسمك ، ولا نعرف كمية البروتين التي ستنتجها بالفعل والتي تسبب هذه الاستجابة المناعية المفرطة النشاط ، ونقول فقط ، “أوه ، نعم ، ستكون بخير ، لا لا تهتم حتى بالاتصال بي إذا كان لديك بعض الألم في ذراعك “.
بالنسبة لي ، هذا أمر محير ، لأنني لا أعتقد أن لديهم أي فكرة عن مدى اختلاف استجابات الشعوب لهذه المعلومات الجينية ، وبالتالي إلى أي مدى قد تكون استجاباتهم شديدة الاختلاف تجاه اللقاح. وهكذا ، بالإضافة إلى هذا القلق العام ، هناك أيضًا لقاحات ناقلات الفيروسات الغدية AstraZeneca و Johnson & Johnson. لذا ، فإن الفكرة هي أننا نتعامل مع فيروس موهن يصيب البشر عادة ، وهو الفيروس الغدي ، ونقوم بتعبئة بعض المعلومات الجينية هناك. وهكذا ، سوف يأخذ ناقل الفيروس هذا الحمض النووي من فيروس كورونا إلى خلاياك ثم يضع الحمض النووي في خلاياك. وبعد ذلك في هذه المرحلة ، لديك المزيد من المضاعفات المحتملة لأنك الآن لا تقوم فقط بإلصاق المعلومات الجينية من فيروس كورونا في جسمك ، ولكن لديك أيضًا مشكلة … مع الفيروس الغدي هناك … ولا أتذكر الاسم التقني لـ ولكن هناك آلية يمكن بواسطتها للفيروسات الغدية أن تتجمع في جسمك.
لذلك ، إذا كنت مصابًا بفيروس غدي ، والذي قد لا يكون حتى من الأعراض ، لأن بعض هذه الفيروسات حميدة جدًا ولا تسبب الكثير من المشاكل. لكن بعضها أسوأ ويمكن أن تسبب أعراض نزلات البرد الشائعة ، ويمكن أن تسبب أيضًا اضطرابات في الجهاز الهضمي ، أشياء من هذا القبيل. ولكن ، لنفترض أنك مصاب بأحد هذه الفيروسات الغدية، فأنت تتعثر بلقاح الفيروس الغدي ، وهذان الفيروسان ، فيروس اللقاح والفيروس من النوع البري ، يعيدان الالتحام في جسمك ويصنعان شيئًا مختلفًا لدينا لا توجد فكرة عما ستفعله ، أو كيف ستتفاعل ، أو كيف ستسبب لك العدوى.
ويمكن أن ينتهي بك الأمر بإنشاء فيروسات خارقة. وهذا أحد الأسباب أنه عندما تم تطوير لقاحات فيروس كورونا في الأصل ، عندما كان السارس شيئًا في عام 2003 ، 2004 ، نظروا في عمل فيروسات حية موهنة. لكنهم قالوا بعد ذلك ، “لا ، لا يمكننا فعل ذلك لأنه يمكنك إعادة اتحاد فيروس اللقاح الحي الموهن هذا مع فيروس كورونا الذي يحدث بشكل طبيعي.” نظرًا لوجود حوالي أربعة أشخاص يصيبون عادة البشر ويسببون أعراضًا من نوع نزلات البرد الشائعة ، لا يتم احتساب فيروس السارس وMERS virus وفيروس السارس 2 الحالي. ولكن ، يمكن أن تتحد هذه الأنواع الأربعة الشائعة مع فيروس لقاح حي موهن (عنصر إلكتروني غير فعّال)، ويمكن أن يخلق ذلك شيئًا لن يكون لدينا أي فكرة عن مدى عدواه أو مدى إصابته. لذلك ، أعتقد أن هذا مصدر قلق أيضًا مع عوامل الفيروسات الغدية التي لم يتم التعامل معها بشكل صحيح في نظر الجمهور.
وبعد ذلك ، أحد الأشياء الأخرى التي وجدتها مثيرة للاهتمام ، كنت أنظر إلى مقطع فيديو آخر كان يروج لتقنيات الجيل التالي هذه ومدى إثارة هذه التقنيات ، “الجميع يهدأ ، لقد عملنا عليها لعقود الآن ، وهم “لم يعد مجرد علامة تجارية جديدة تمامًا ، لقد فكر شخص ما في هذا الأمر”. وبصفتي باحثًا ، عند سماع ذلك ، “لقد عملنا على هذه منذ عقود.” لا يعني ذلك أنهم آمنون ، فهذا يعني أننا لم نحقق نجاحًا منذ عقود في هذه الأشياء. هذه هي الرسالة الحقيقية التي يتم نسجها بطريقة إيجابية ، إنها مثل ، “أوه ، لدينا خبرة في هذا في المختبر.” لدينا خبرة في ذلك لا تعمل ، هذا ما لدينا.
JHW: إذن ، أحد الأشياء التي تحدث هي أن معظم الناس يعرفون ولكن، الشركات التي أنتجت تلك اللقاحات لا يمكن مقاضاتها. وستجني الشركة أرباحًا من صنعها على أي حال ، وحصلت على أرباح من تطويرها لأنه طُلب منهم القيام بذلك في ظل برنامج Warp Speed وبملايين ومليارات الدولارات…
PA: هذا في الواقع … مطروحًا منه التمويل المسبق لـ Warp Speed ، هذا هو الوضع الفعلي لجميع اللقاحات التي تم تطويرها في الولايات المتحدة. يتم تعويض جميع مصنعي اللقاحات ضد المسؤولية عن منتجاتهم ، وسيتعامل برنامج تعويض إصابات اللقاح ، VICP ، مع أي مطالبات بإصابة اللقاح. وقد تحدثت عن هذا قليلاً في كتابي أيضًا. ومجرد تحليل بعض الأرقام بناءً على العدد الفعلي للتقارير السلبية التي تم تقديمها بالفعل إلى VAERS ، وهو نظام الإبلاغ عن الأحداث الضائرة للقاح ، استنادًا إلى حقيقة أن هذا ربما يكون أقل بكثير مما يحدث بالفعل. نظرًا لأن معظم الأشخاص لا يفكرون في تقديم شيء ما ، لأنهم يعرفون أنه من المستحيل توصيله مؤقتًا ، أو أن في بعض الحالات يعرفون فكرة وجود اتصال للقاح.
نظرًا لأن الكثير من الأحداث السلبية التي تحدثت عنها في الكتاب تكون شائعة جدًا أو محتملة مرتبطة باللقاحات ، فمن الصعب للغاية تحديدها من حيث التسلسل الزمني الفعلي لها ، وتطورها ، وبداية ظهورها. لأن الكثير منهم يعانون من الحساسية أو استجابات المناعة الذاتية لأنك تحرض الاستجابة المناعية بطريقة غريبة جدًا في الواقع. عندما تقوم بتلقيح نفسك ، فأنت لا تعرض نفسك لمسببات الأمراض من خلال المسار الطبيعي ، فأنت تمر في عضلاتك بدلاً من فمك. في بعض الحالات تصيب نفسك بثلاثة أو أربعة أو خمسة أو عشرة أمراض في نفس الوقت. لن تصاب مطلقًا بالحصبة والنكاف والحصبة الألمانية وشلل الأطفال والجدري المائي والدفتيريا والتيتانوس والسعال الديكي في نفس الوقت ، ولكن قد تحصل على كل هذه اللقاحات في زيارة واحدة للأطباء.
لذلك ، هناك الكثير من المشاكل من حيث تحديد عدد الأحداث الضائرة المرتبطة باللقاحات بشكل عام. لكن مصنعي اللقاحات ليسوا مسؤولين ، وأعتقد أنه سيكون هناك … كان هناك نوع من الحماية الخاصة الممتدة خصيصًا للقاحات COVID. لأنه ، إذا من الواضح أنك تسرع في إنتاج شيء ما ، أعتقد أن هناك نوعًا من المسؤولية التي قد تظل تتحملها ، حتى كشركة مصنعة للقاحات بشكل عام. ولكن نظرًا لأن هذه حالة طارئة الآن حيث تم منحك ترخيصًا للمضي قدمًا والقيام بذلك ، وخفض الاختبار الخاص بك إلى … علمت اليوم أن شركة Moderna قد طلبت ردود فعل سلبية لمدة سبعة أيام. وتعلمت أيضًا اليوم ، أنه نظرًا لأنه لا يعتبر من الأخلاقي عدم إعطاء شخص ما لقاح فيروس كورونا إذا كان لدينا لقاح فيروس كورونا “فعال” ، فإن شركة Pfizer تقوم بالفعل بتلقيح مجموعة الدواء الوهمي الخاصة بهم بلقاح فعال فعلي.
لذلك ، لن يكون لدينا المزيد من البيانات حول التأثيرات طويلة المدى من هذه اللقاحات ، لأننا لن نمتلك مجموعة الدواء الوهمي بعد الآن ، لأنهم سيمضون قدمًا ويحصلون على اللقاح. وهو ما يثير دهشتي كباحث وهو … كيف ترتكب هذا المستوى من … إنه احتيال علمي ، حقًا ، أن تقول فقط ، “نحن فقط نقضي على مجموعتنا الضابطة. نحن فقط نخرجهم تمامًا من الوجود ، لذلك ليس لدينا الآن طريقة لنقول مدى أمان هذا اللقاح في الدراسات طويلة الأجل “.
JHW: أحد الأشياء الأخرى التي قصدت أن أسألك عنها ، وقت أخذ اللقاح إلى وقت مواجهة الآثار ليس فوريًا. ما الذي نتحدث عنه هنا؟ هل هو يوم ام يومان؟ او ما هو؟
PA: حسنًا ، هذا يعتمد على نوع رد الفعل الذي تراه. إذا كنت تعاني من الحساسية المفرطة ، وهو رد فعل يحدث مع بعض اللقاحات ، فهذا هو رد الفعل التحسسي حيث تبدأ مجاري الهواء في التقريب وأنت في خطر الموت من رد فعل تحسسي شديد. من المفترض أن يحدث ذلك ما يقرب من جرعة واحدة من بين مليون جرعة من لقاحك العادي. يحدث ذلك بمعدل 22 مرة أكثر من لقاحات COVID ، لذلك أعتقد أنه واحد من بين 45000. وهذا مرة أخرى ، ليس معدلًا مرتفعًا بشكل رهيب ، ولكنه يزيد 22 مرة عن متوسط اللقاح الذي تم تطويره بشكل طبيعي. ويجب أن يكون هذا مخيفًا ، لأنه إذا كان الناس يعانون من الحساسية المفرطة ، وهو رد الفعل الأكثر خطورة الذي يمكن أن تتعرض له من اللقاح ، 22 مرة أكثر مما يعانون منه من لقاحك العادي ، فماذا يعني ذلك عن الآثار الجانبية الضارة الأخرى؟
وهكذا ، أن شلل الوجه النصفي Bell’s palsy هو أحد الآثار الجانبية الضارة. نحن نشهد الشلل، مع لقاح فايزر ومودرن ، لقد رأوا ذلك بشكل متكرر في السكان الذين تم تلقيحهم أكثر من السكان غير الملقحين. بالطبع يريد الجميع التقليل من شأنها والقول ، “يتم حل معظم حالات شلل الوجه النصفي في غضون ستة أشهر”. لكن ليس كل شيء. وفقدان السيطرة على عضلات الوجه لا يكون دائمًا شلل Bell’s palsy ، بل يمكن أن يكون أيضًا من أعراض اضطرابات عصبية أخرى أكثر إشكالية. مثل متلازمة Guillain-Barre ، التي يسارع الجميع إلى قولها ، “لم نر أي حالات لمتلازمة Guillain-Barre.” حسنًا ، منذ متى وأنت تختبر ردود الفعل السلبية ، 28 يومًا؟ لا أعرف ما إذا كنت ستشاهد متلازمة غيلان باريه في غضون 28 يومًا ، فهذه متلازمة تستغرق وقتًا أطول للتطور. لذا ، فإن أمراض المناعة الذاتية ، كقاعدة عامة ، تستغرق وقتًا أطول لتتطور.
وهناك بعض الأدلة على أن داء السكري من النوع الأول هو أحد الآثار الجانبية المحتملة للتلقيح. قد يستغرق ذلك عامًا حتى يتطور بشكل كامل ، بمجرد أن يبدأ جسمك في مهاجمة خلايا البنكرياس. قد يستغرق وقتًا طويلاً جدًا للتطوير. يمكن أن يستغرق الألم العضلي الليفي وقتًا طويلاً جدًا حتى يتطور.
ولكن بعد ذلك ، هناك أشياء أخرى ، أكثر ردود الفعل السلبية الشديدة شيوعًا ، على الأقل بالنسبة إلى Moderna ، يعاني سبعة و 7.5 أو 8 ٪ من الأشخاص من إجهاد شديد بما يكفي لمنعهم من ممارسة أنشطتهم اليومية العادية. وأعتقد أن حوالي 6٪ يعانون من الصداع الشديد. وكان هناك بعض الأشياء الأخرى التي كان الناس يعانون منها [غير مسموع 00:50:44] والتي يمكن أن تحدث في غضون يوم أو يومين ، أو حتى على الفور من اللقاح. لذلك ، يعتمد فقط على رد الفعل العكسي.
أكثر ما يقلقني هو تلك الأشياء المزمنة وطويلة المدى في اتجاه مجرى النهر. ولدي اهتمام خاص بهذا لأن عائلتي لديها تاريخ حالة مثير للاهتمام للغاية لجميع أنواع مشاكل المناعة الذاتية ، من جيل جداتي إلى أبناء شقيقاتي. وسواء كانت هذه كلها مرتبطة باللقاحات أم لا ، لا أستطيع أن أقول ، وبالتأكيد لا أعتقد أن جيل جداتي ربما كان هو الحال لأنهم لم يتلقوا جرعات كثيرة في ذلك الوقت. لكنني أعلم أنه إذا كانت اللقاحات يمكن أن تؤدي إلى أمراض المناعة الذاتية ، ومن الواضح أنني أمتلك علم الوراثة لمشاكل المناعة الذاتية ، فأنا لا أتناول لقاحًا غير ضروري ، فهذا ليس بالذكاء. ولكن هذا هو الجزء الذي يقلقني أكثر ، لأن هذه الأشياء لن تظهر إلا بعد التطعيم بالفعل ، فمن يعرف عدد الأشخاص. إذا كان الأمر سيستغرق من ستة أشهر إلى عام ، إلى عدة سنوات حتى تتطور هذه الحالة المرضية حقًا ، ومن ثم يصعب جدًا ربطها باللقاح الأصلي في بعض الحالات.
JHW: حذرت حكومة المملكة المتحدة النساء الحوامل من تناوله. حذرت إدارة الغذاء والدواء والوكالات الأخرى من أن أولئك الذين يعانون من الحساسية تجاه مكونات اللقاح يجب ألا يأخذوها. كان هناك تحذير من أن الرجال قد يفكرون في تجميد حيواناتهم المنوية قبل أخذها بسبب نوع من الخوف من التأثير المحتمل بهذه الطريقة. ماذا عرفتي عن تلك الاحتمالات؟ هل هذا مصدر قلق للخصوبة أيضًا؟
PA: أود أن أكون قادرًا على تقديم إجابة نهائية عن ذلك ، ولا يمكنني ذلك. وجزء من سبب عدم تمكني من ذلك هو وجود الكثير من المعلومات المتضاربة التي يتم تداولها. وحتى مع الخبرة التي أمتلكها ، لم أتمكن من تكوين رؤوس أو ذيول كافية لأكون قادرًا على قول بطريقة أو بأخرى. سأقول أن الحكومة البريطانية تصدر هذا التحذير جزئيًا ، لأنه لم يتم إجراء أي اختبار على النساء الحوامل. لذلك ، لا تعطي لقاحًا لمجموعة حساسة لا يوجد عليها اختبار سلامة ، بشكل عام ، هي الفكرة هناك. لا أعتقد أن هذا يتم بدافع أنهم يعرفون شيئًا عن الخصوبة لم يقولوه ، لقد خرجوا وقالوا ، “لم يتم إجراء أي اختبار، لذا لا ينبغي لنا القيام بذلك.”
ولكن كانت هناك بعض المعلومات التي تم تداولها والتي تقول ، “لا تحصلي عليها إذا كنت تخططين للحمل في غضون الشهرين المقبلين.” الذي بدا غريبًا جدًا بالنسبة لي ، لأنه ليس شيئًا تم إصداره مع لقاحك العادي. وإذا كان يسبب مشاكل في الخصوبة ، فمن المؤكد أنه لن يكون أول لقاح يسبب مشاكل في الخصوبة.
كان هناك عدد من اللقاحات التي طورتها منظمة Word Health والتي كان من المفترض أن تسبب العقم عن قصد. لقد كانوا يبحثون عن لقاح لتحديد النسل منذ السبعينيات. لقد اختبروا نساء غير مطلعات وغير موافقين في كينيا والفلبين والمكسيك ، وأعتقد أن دولتين من دول العالم الثالث. وقد تحدثت شخصيًا مع طبيب في كينيا ، والذي كان أحد الذين حددوا أن لقاحات التيتانوس التي كانت تُعطى للنساء الكينيات ، ونستهدف على وجه التحديد النساء في سن الإنجاب ، كانت مصابة بـ hCG. والتي ، إذا قمت بحقنها بالتزامن مع ذوفان الكزاز ، يمكن أن تجعل النساء عقيمات لفترة غير محددة من الزمن. لذلك ، هذا شيء تم القيام به في الماضي ، سرا ، وأعتقد أن هذا جزء من سبب قلق الكثير من الناس.
ومن ثم يرتبط لقاح جارداسيل Gardasil ، وهو لقاح فيروس الورم الحليمي البشري ، بانخفاض مخيف في الخصوبة. وهناك دراسة أجريت على النساء ، على ما أعتقد ،تتراوح أعمارهن بين 25 و 29 عامًا ممن تلقين أو لم يتلقين اللقاح ، لذلك لم تكن هذه تجربة تم إجراؤها ، لقد كانت مجرد النظر في البيانات بعد ذلك. والنساء اللواتي تلقين الجرعات الثلاث من لقاح فيروس الورم الحليمي البشري كان ثلثهن أكثر عرضة للحمل والولادة مثل النساء في نفس الفئة العمرية ، مع تعديلهم تقريبًا للمشكلات الطبية الأخرى التي يمكن أن تؤثر على الخصوبة. كان احتمال الحمل لديك ثلاثة أضعاف إذا لم تكن قد تلقيت اللقاح مطلقًا ، مقابل ما إذا كنت قد تناولت الجرعات الثلاث. هذه أمور مثيرة للقلق ، لأنه لم يتم إخبارك بهذا …

JHW: بالتأكيد.
PA: … عندما تدخل ويقول طبيبك ، “هل ترغب في أن تحصل ابنتك على جارداسيل؟ Gardasil ” لم يتم إخبارك بأنها قد تصاب بأمراض المناعة الذاتية الرهيبة التي ارتبطت بها ، بما في ذلك متلازمة التعب المزمن ومتلازمة تسمى PoTS. ولا يمكنني أن أتذكر أبدًا ما يمثله PoTS ، لكن من المروع أن يكون لدي ذلك ، أعرف بعض الأفراد الذين يفعلون ذلك وهو مقيد جدًا لهم ، إنه مرض في القلب. وبعد ذلك ، لم يتم إخبارك أيضًا ، “وملاحظة قد لا تتمكن أبدًا من إنجاب طفل “.
JHW: دعنا نتطرق قليلاً إلى ما إذا كان لقاح COVID ضروريًا ، وبعد ذلك سأطلب منك إعطاء بعض الأفكار النهائية.
PA: هل لديك سؤال محدد حول ذلك أم بشكل عام فقط؟
JHW: عندما تنظر إلى اللقاحات ، يتعلق بما إذا كانت ضرورية أم لا. تحدثنا عن السلامة ، وتحدثنا عن الأخلاق ، وتحدثنا عن الفعالية ، ولكن هل هناك حاجة فعلاً؟ وهذا ينظر إلى وضعنا الحالي مع COVID الآن.
PA: تحدثنا قليلاً عن معدل الوفيات ، ومعدل الوفيات منخفض جدًا جدًا. متوسط عمر الوفاة أعلى من متوسط الوفيات المتوقع في الولايات المتحدة. نحن لسنا في وضع يبدو أنه ضروري ، ويبدو أن مخاوف السلامة تقابل الفوائد ، من حيث أعتقد أنه من المرجح أن يكون لديك رد فعل سلبي تجاه اللقاح ، فأنت ستصاب بـ COVID ، ناهيك عن للموت من COVID. ولكن أيضًا ، لم يزعم أحد … أو لم يذكروا ذلك بذكاء أثناء الترويج لمجالات أخرى من النجاح ، لكن لم يزعم أحد أن للقاح سيؤدي في الواقع إلى توقف الفيروس عن الانتشار. الادعاءات الوحيدة التي قدمتها كل من شركة Pfizer و Moderna هي أنه “إذا حصلت على اللقاح ، فستقل احتمالية إصابتك بأعراض COVID الشديدة مما لو لم تحصل على اللقاح.” ومرة أخرى ، فهم ينظرون إلى جزء بسيط..
لذلك ، قامت شركة Pfizer بتلقيح 43000 شخص وفحصوا ما يقرب من 200 شخص ظهرت عليهم الأعراض. ثم قامت شركة Moderna ، بنفس الشيء ، بتلقيح 30 ألف شخص ، ونظروا إلى ما يقرب من 200 شخص ظهرت عليهم الأعراض. وبعد ذلك قدم كلاهما ادعاءات أن لقاحاتهما كانت فعالة بنسبة 90٪ ، بناءً على حقيقة أنه ، “حسنًا ، الأشخاص الذين ظهرت عليهم الأعراض ، 90٪ من الأشخاص الذين ظهرت عليهم أعراض أسوأ ، كانوا في المجموعة غير الملقحة.” لم يختبروا ما إذا كان هؤلاء الأشخاص إيجابيين لفيروس سارس كورونا ، ولم ينظروا إلى أي أعراض أخرى ، ولم ينظروا ، “على المدى الطويل ، هل يمنعك هذا بالفعل من تطوير الأعراض على مدى فترة زمنية أطول؟” وقد نظروا خلال فترة أسبوعين فقط ، كما قلنا. لم يختبروا أيًا من الأشياء التي كان ينبغي عليهم اختبارها ، من حيث تحديد ما إذا كان هذا اللقاح وقائيًا أم لا.
لذلك ، ليس لدينا أي سبب للاعتقاد بأن هذا اللقاح سيفعل أي شيء لإبطاء انتشار الفيروس. ويقول أشخاص مرموقون جدًا ، “احصل على اللقاح ، واحصل على اللقاح ، لكن استمر في ارتداء قناعك لأنه لن يؤثر في الواقع على الانتقال.” لماذا إذن أحصل على اللقاح؟
JHW: بالضبط. وكيف تجرؤ أن تقترح أنه من أجل السفر ، من أجل إعادة المجتمع إلى طبيعته ، تحتاج إلى لقاح ، لأن ذلك لا معنى له على الإطلاق.
PA: السبب الوحيد الذي يجعلني أحصل على لقاح COVID هو لمصلحتي الخاصة لهذا التأثير الوقائي المتواضع ضد تطوير أسوأ الأعراض الممكنة. بالنسبة لي ، أنا لست في مجموعة عالية الخطورة ، وليس لدي أمراض مصاحبة ، وليس هناك سبب لي للحصول على هذا اللقاح ، ولن يساعد جاري. إنه ليس “الشيء الصحيح الذي يجب فعله” أو الشيء الأخلاقي الذي يجب القيام به ، أو الشيء الضروري الذي يجب القيام به لأي شخص آخر غير نفسي. وإذا لم يكن ذلك ضروريًا بالنسبة لي ، فليس من الضروري إطلاقًا التقاط هذه اللقطة.
JHW: باميلا ، قبل أن أسألك عن أفكارك النهائية قبل أن ننتهي ، أردت أن أشكرك نيابة عن جميع مشاهدي موقع LifeSite. أعلم أن الكثير من الأشخاص يطرحون أسئلة ، وقد تلقيت منك إجابات أوضح مما رأيته في أي مكان من قبل ، لذا شكرًا لك على ذلك. كتابك بعنوان التطعيم: منظور كاثوليكي ، أين هو متاح؟
PA: إنه متاح على موقع Kolbe Center على الويب ، لذا فإن Kolbe مثل [غير مسموع 00:59:21] ، K-O-L-B-E ، C-E-N-T-E-R dot org.
JHW: سنقوم بربطه في منشور مدونتي وفي وصف هذا الفيديو أيضًا. ولكن ، اعطنا إذا أردت يا باميلا ، تأملاتك النهائية حول هذا السؤال.
PA: الشيء القصير هو عدم فهمه ، إنه ليس جيدًا لروحك وليس جيدًا لجسدك. وأعتقد أننا نحتاج حقًا ، ككاثوليك ، إذا لم نقف الآن … نحن نفقد الفرص التي سنضطر إلى الوقوف عليها وتصحيح هذا الخطأ الذي يحدث الآن منذ عقود. وهو مستمر منذ عقود وسنكون مسؤولين عن ذلك. عشنا في هذا الوقت ، كانت لدينا فرصة للوقوف ، وأتيحت لنا الفرصة للقيام بشيء ما ، وإذا لم نفعل ذلك ، فسنحاسب على ذلك في النهاية. لا يمكنك الجلوس على يديك فقط والقول ، “حسنًا ، لن آخذه. حسنًا ، إنها ليست صفقة كبيرة “. هذه صفقة كبيرة ، هذا تل يستحق الموت.
JHW: آمين. وقد تم إعطاؤك بعناية شديدة للقيام بهذا العمل ، لبدء ذلك قبل أن يكون واضحًا جدًا أنه كان في أمس الحاجة إليه ، ويظهر الآن كما لو كان مخططًا له. بارك الله فيك على ما فعلته والوضوح الذي قدمته.
PA: شكرا جزيلا لك.
JHW: وبارك الله فيكم جميعًا. سنراكم في المرة القادمة في برنامج جون هنري ويستن
‘A hill worth dying on’: Expert explains how aborted baby cells taint COVID vaccines
Pamela Acker, a vaccine researcher, shows how the process by which the COVID vaccines are developed is like ‘what the Aztecs used to do.’
Editor’s note: The following is a rough transcript of LifeSite co-founder John-Henry Westen’s explosive interview with Pamela Acker, a vaccine researcher and expert.
John-Henry Westen: Welcome to this episode of the John-Henry Westen Show, where I am very pleased to bring you Pamela Acker, who is a researcher into vaccines, in fact she’s published a new book called Vaccines: A Catholic Perspective. And we are going to get into the most controversial topic going on today, we’re going to be talking about what Bishop Athanasius Schneider said, what the actual case is about abortion tainted vaccine, including the COVID vaccines, you’re going to want to stay tuned.
Let’s begin as we always do at the sign of the cross. In the name of the Father and of the Son, and of the Holy Spirit, Amen. Pamela Acker, welcome to the program.
Pamela Acker: Thank you very much, it’s my pleasure to be here.
JHW: If you can start, just tell us a little bit about yourself, about your background in this area of vaccinations.
PA: I’ve never liked to be on the cutting edge of anything, so I was excited about vaccines about 20 years ago, before it became a hot COVID topic. But, when I was in high school I was interested in studying biology, and I was particularly interested in studying it because at the time there was some thought that plants could be genetically engineered to deliver vaccines. And there was two things about that that I found very exciting, one was that you could eat something instead of get stuck by something, because nobody likes hypodermic needles. And the other was that this might make it easier to distribute vaccines in third-world countries, because you wouldn’t have to worry about special refrigeration or perishable components, you could just grow them on site.
d then, I pursued a master’s degree at Catholic University of America in 2010, 2012, I actually was there for my PhD, but left with a master’s because the lab that I got into, which was also involved in vaccine development, was working on a project for HIV vaccines. And the grant funding was under the The Bill & Melinda Gates Foundation, we had gotten the first stage of our grant, we were ready to apply for the second stage and trying to produce enough results to show that our plan was tenable there.
There was a lab meeting that we were all sitting around at, and my primary investigator said, “Look, everybody’s got to get onboard with this particular aspect of the project.” Which belonged to a colleague of mine. And so, I turned to her and I said, “What are you doing this part of the project in?” And she said, “HEK-293 cells.” And this point most people have heard of these because they are connected with the COVID vaccines, but at that time I hadn’t. So, I asked her what HEK stands for, and she told me, “Human Embryonic Kidney.”
And then I spent a couple of weeks researching what that meant and what that entailed, and I came across the work of Alvin Wong from The National Catholic Bioethics Center, who wrote an article in… I believe it was 2005 or 2006, called The Ethics of HEK-293. And his work helps me a lot to discern whether I could actually be involved in this project or not. And when I expressed my concerns to my primary investigator, it ended up being the end of my career in his lab.
So, I did not get my PhD, I left with my master’s. But, the use of aborted fetal cells in vaccines is definitely an issue that’s near and dear to my heart, and it’s influenced a lot about my life up to this point. But, I also was able to be in the lab for about nine months before that ethical issue was raised, so I have some direct research experience on vaccine development that comes into play. And it has enabled me, I think, to have a unique voice in this argument right now.
JHW: Absolutely. So, eminently qualified to discuss this topic more than most, having worked inside a lab as well on vaccines. Also, someone who has now written a book on this. We’re very early into the COVID thing to have already written a book on this, that was quite something, how’d you manage that so quickly?
PA: Again, I don’t like to be on the cutting edge of anything, so I started that book two years ago, almost. It was taking the trash out one fateful winter night, and fell and sprained my ankle, and unlike a normal person, I never got better. So, I was laid up on the couch for a very long time, and [inaudible 00:05:25] Kolbe Center had been after me to look into the issue of vaccines for a while. And, when I was on the couch with nothing better to do then read all the things that nobody has time to read, was when I actually started the research for this book.
So, I actually started around April of 2019, so before COVID was ever an issue, hence the reason that the book was so well timed.
JHW: Well, that’s really providential. So, we are in an absolutely crazy time because the issue of vaccines, which has been around for many decades now, has taken on an absolutely new urgency with what seems basically like it’s going to be forced on everyone. Even though almost everyone’s saying, “No, no, we’d never force it.” In reality, they’re already talking about, “You need to be vaccinated to take a flight, you need to be vaccinated to go into a store.” We’re already seeing with the mask mandates and the social distancing mandates, the lock downs and everything else, that they are really willing to take draconian measures. So, while you might not be forcibly held down and vaccinated, you’re life will become unmanageable if you don’t take it.
So, this is our situation. Now, when we’re looking at taking vaccines, as a parent we’ve assessed things like, “Is it necessary? Is it safe? Is it effective?” But also one of the questions is, “Is it moral?” And so, I’d love to address all of those points with you, with regard to the COVID vaccines that are now approved, and what does it mean that they’re abortion tainted? So, if we could start right in with the abortion tainted, because I think for most people, one of the qualifying factors to take a vaccine in the first place will be its moral nature. “Is it moral to take this? What are they?” So, why don’t we start with the two currently approved vaccines for Coronavirus, for COVID. What are they? And how do they differ?
PA: The two vaccines that are currently approved are the Moderna vaccine and the Pfizer vaccine, and they’re both mRNA vaccines, and so at a molecular level they’re very similar. Both of the vaccines were made using a biotechnology technique that can synthesize nucleic acids in the laboratory. So, a lot of people are trying to argue that they’re moral because the mRNA that’s made never touches fetal cells. But that’s not the whole of the story when you look at the way that these vaccines were developed.
And so, the original research papers document the use of HEK-293 cells in producing these vaccines. And so, they were used in two different ways. One is that the spike protein that the mRNA codes for… can just do a three minute crash biology course. mRNA is messenger RNA, it’s the nucleic acid that’s a copy that’s made of you DNA, and then it’s sent out to the ribosomes in the cells and protein is produced using that messenger copy. So, what the vaccine reports to do is to take messenger RNA that codes for the spike protein of Coronavirus and insert that into your cells so that your human cells will then make the spike protein from the Coronavirus.
And the thought is that this is going to be a very effective way to vaccinate you because we found that if you just take the spike protein and inject it into people, it tends to degrade too rapidly for a good immune response. You tend to have some other complications which I’ll touch on a little bit later in the interview. But, the thought is that if your body’s making it itself, then you can get a prolonged enough exposure to the spike protein that you’ll be able to mount an immune response to it. So, that’s the basic way that it’s supposed to work.
So, the spike protein by itself is, in the words of one researcher, kind of floppy, it doesn’t tend to keep its shape very well. And so, scientists genetically engineered a spike protein that will keep its shape, it’s got some mutations that cause it to be stabilized. And so, this original design of this protein… so, when they originally mutated it… they needed to see if it would actually keep its shape correctly, if that would correct the floppiness problem. So, they took that genetic information, and they transformed cells to produce the spike protein so that they could purify it and take a look at it using techniques for visualizing the 3D structure of proteins. And that original experiment was done in HEK-293 cells. So, the spike protein that the vaccines code for, was originally developed, effectively, in aborted fetal cells.
And an additional way that aborted fetal cells were used in the project is, before they were going to inject this mRNA into a human being to see if you could get human cells to make Coronavirus spike protein, you would want to test that in cell culture, you would want to test that in a laboratory. Because, it’s a lot less expensive and dangerous than testing it in a human being. And so, if you can’t even get the cells in a laboratory to make it then you probably can’t get a human body to make it. So, the cells that then this was tested in were also HEK-293 cells. And this has all been published in the literature, and I’ve read a couple of the papers documenting that both of these vaccines used HEK-293 in their testing.
And, a lot of people want to say, “Well, that was just done to develop the vaccine in the very beginning, so the research part… so, it was a one and done kind of thing, it’s no big deal.” But just recently, Stacy Trasancos posted an article, which is available on Children of God for Life website, and she pointed out… and as a researcher I can confirm she’s absolutely right, that these things also have to go through quality control testing. So, every time I make another batch of the mRNA, which is synthesized using a laboratory technique, then I need to test and make sure it’s still viable, that’s a fairly common thing, to have quality control like that in the laboratory.
So, the testing with these aborted fetal cells may actually be ongoing in the production of these vaccines. Because generally, when you scale up production of vaccine beyond your research and development, you’re going to use the same testing procedures to test the scale up that you use to test your smaller batch, unless it’s for some reason not feasible. But, this is a very feasible way to test this for these researchers. It’s not a moral way, but it’s very feasible because these cells have been optimized for use in a laboratory. And they’re almost ubiquitous in tissue culture research, unfortunately there’s a lot of laboratories around the world that use these HEK-293 cells. And there’s specific products that are basically optimized for them to have ideal growth conditions. So, there’s a whole industry based on these aborted fetal cells in basic science research that I think people aren’t super familiar with.
JHW: So, just to be clear, both the COVID-19 vaccines, both the Pfizer and the Moderna we both, not only developed in its spike protein with HEK-293, the aborted fetal cell line, but also in their initial testing. And now you’re telling us, at least from this article from Stacy Trasancos, in ongoing testing currently for new batches.
PA: Yes. As far as I know there is ongoing testing currently for batches. That is not published in the literature per se, because non of the data post the initial clinical trials has been published, but there’s substantial reason to think that this is going on.
JHW: Let’s stop there for a second and just do a bit of a rewind for people, because I think people have to understand something about HEK-293 and PER.C6 and a bunch of the other aborted fetal cell lines that are at work here. And that has to do with their initial development anyway, because I think a lot of people are under the impression that… not anymore now, since you’ve already said what you’ve said with regard to the use of HEK-293. But, I think a lot of people are under the impression, “Well, that was one baby killed way back in the 1970s and it’s so remote from that date right now, and that’s an acceptable thing we just have to live with because it’s saving so many lives.” If you can unpack for us, what is HEK-293 exactly? And was it just one baby that accounts for it, and what about all the other fetal cell lines?
PA: There are a number of fetal cell lines in existence right now, and I’m just going to read off a few of them for you here from Children of God for Life. There’s WI-38, MRC-5, HEK-293, PER.C6, there’s another one that I’m forgetting the name of that was developed in 2015 that’s not currently being used in any vaccines, but has a potential to be used in vaccines and is used in other therapeutic treatments. So, there’s a number of these cell lines that are currently being used to develop a variety of therapeutics, everything from vaccines to treatments for Cystic fibrosis.
Most people, as you say, hand wavingly dismiss it and say, “Oh well that was one baby that died, we can’t go back and undo it, we might as well get something good out of it now.” Which of course, violates the principle of the integral good, and the fact that you simply can’t use the ends to justify the means. But I’m not a moral theologian, so I’ll stick to the science.
For, HEK-293, that was… one of things that I’ve seen come up a couple of times in articles I’ve looked at about the ethical considerations that are involved, is that people say, “Well, there wasn’t documentation that that was an elective abortion, so it could have been a spontaneous abortion.” And this is a bit disingenuous or ignorant on the part of these authors, because in order to produce a viable cell line, there’s a number of things that go into that, and it’s a very difficult thing to do.
And so, I was doing some research specifically on HEK-293 to prepare for this interview, and the number system that’s involved there… the HEK stands for Human Embryonic Kidney, but 293 stands for this is the 293rd experiment that this particular researcher did to develop a cell lines. And that doesn’t mean that there were 293 abortions, but for 293 experiments you need far more than one abortion. And we’re talking probably 100s of abortions. And, this was done with the collaboration of some hospitals. And there was a group in Sweden that was involved in developing the WI-38 cell line, so a different cell line, but they routinely were aborting babies for the use in trying to develop fetal cell lines.
So, people at this point usually have the question of, “But why? Why a fetal cell line?” And, when you try to grow cells in culture in the laboratory, they go through a process called immortalization, to develop a cell line. And people kind of confuse that, because it sounds like they live forever, with thinking that you can make these cells live forever in a laboratory. You can’t. You can make them live a lot longer than primary cell culture, if you were to just take something out of my arm and put it to grow in a Petri dish, it would survive for a few sub divisions, but not very many. But, if you introduce some mutations into it, it can survive for a lot longer. And so that’s what you have when you have an immortalized cell line, you have something that’s been mutated usually with viral oncogenes. And these are genes that promote cancer actually, and so put a bookmark there too because this is important to something that hopefully we’ll discuss a little later in the interview, about some of the dangers of using… just the biological dangers, let alone moral dangers of using the aborted fetal cell vaccines.
The immortalized cell lines are often given cancer promoting genes that disrupt the function of cancer suppressor genes, or tumor suppressor genes. And so, they can grow, not completely indefinitely, but for a lot more generations in a laboratory. If you start with adult cells, you have basically a shorter shelf life, because adult cells have already undergone a certain number of cell divisions, and so that kind of counts towards the total number that they could actually undergo. And so, if you use adult cells in a laboratory, you will have a shorter lifespan for your cell line, you’ll have to develop a new cell line sooner, and it’s not as commercially viable. If you start with embryonic or fetal cells, you have the maximum lifespan available for your cell line, and so that I think was probably one of the things that was used to justify the use of these aborted fetal cells to begin with.
And then, another question people have is, “Well, why couldn’t HEK-293 have been just a spontaneous abortion? Why couldn’t it just been a miscarriage? Because, the hospital lost the documentation about this particular baby that was used to develop the cell line, and so we don’t really know whether it was an elective abortion or a spontaneous abortion.” Well, we have all the reason in the world to think it was actually an elective abortion that was done on purpose, because the researchers who have been involved in this sort of thing have gone on record saying basically that, “You need to get that tissue within about five minutes of the abortion in order for it to be optimally viable, and if you wait an hour, it’s useless.”
So, if we’re talking about a spontaneous miscarriage, this baby dies long before the fetal tissue is removed from the body of the mother. That spontaneous abortion or that miscarriage would not be viable to start a cell line at all, there’d be no way that you could get a living cell line out of dead tissue. So, this had to have been a baby that was aborted and they knew that that tissue was going to be used for research so they could get there within that five minutes to an hour window, preferably within the first five minutes, in order to get that tissue preserved.
JHW: Wow, so that goes right into the baby part scandal that we’re dealing with now, where university researchers ask the mother first, “We’re looking for a kidney or an arm or whatever to experiment with, so when you’re going to have your abortion anyway, can you do this?” And sometimes ask them to wait longer so it’s further developed, so that they’ll have a better specimen. Absolutely sickening. So, this went on even with the vaccines, that this was not only a planned abortion, this was a planned abortion and extraction of fetal tissue [inaudible 00:20:31] used within five minutes of the abortion. So, the nonsense about it being a miscarriage is totally shown.
PA: I was going to say it’s even worse than that because… and this is where I always issue a warning, if there are any little ears listening to me talk on a recording, because it’s a lot more graphic even than what I’ve just described. Because, in a lot of cases, the babies… because it is done on purpose for research purposes, so they will actually deliver these babies via cesarean section, the babies are in some cases still alive when the researchers start extracting the tissue. To the point where their heart is still beating, and they’re generally not given any anesthetic because that would disrupt the cells that the researchers are trying to extract. So, they’re removing this tissue while the baby’s alive, and in extreme amounts of pain, and so this makes it even more sadistic.
And my Pastor just recently gave a sermon likening this to what the Aztecs used to do, when they would consecrate their temples, they would literally rip out the beating hearts of the victims that they were slaying on top of the temples, and then cast their bodies down the side. This is pretty much exactly the same thing that these researchers are doing.
JHW: Yeah. And you had mentioned, we’re getting out the Human Embryonic Kidney, HEK, so it’s the kidney that they have to access. So, they’re cutting open these live babies, just delivered by cesarean section… yes, and they’re too young perhaps to live outside the womb by themselves right away, but they’re still alive enough, and we already know that they’re feeling pain. And then, they open them up to take… that has to be known. Because, I think a lot of the determination of the morality of these things, even morality as separated by years and so it’s remote connections, as they call it, I don’t think that they took into consideration what this actually is. That’s why the science that you’re presenting here is so incredibly important, because the people who made those determinations… and we all know…
And let me just explain, that in 2005, the Vatican first, through the Pontifical Academy for Life, came out with a document saying that, the use of such vaccines, if there is no others available, and if your objection to the procedure of how it was developed is known, and if it’s needed, is morally acceptable somehow. But, even at that time… this was 2005 and then it was rubber stamped, I guess, in 2008 with the CDF. However, I don’t know that these facts were known at that time. And if they were, it’s absolutely unbelievable. So please, continue.
PA: Sure. So, since you referenced the document by the Pontifical Academy for Life, I do address that in the book that I wrote on vaccination, and there’s some real problems with the science that was presented to the people who were making those decisions. Because, one of the strongest points that they used to justify the position that they take, in terms of, “These vaccines can be permissible if the situation is sufficiently grave,” is the incidents of congenital rubella syndrome.
Now, congenital rubella syndrome is no laughing matter, this is when a baby contracts rubella from its mother in utero in the first trimester, and it can result in blindness, deafness, mental slowness, and even stillbirth in the infants, so it is a serious disease. Now, rubella itself is not a particularly serious disease, particularly if contracted in childhood, most people won’t even have symptoms. And I think over half of the cases, nobody even makes a trip to the doctor because there’s nothing noticeable or going on. And so, this is a very mild disease in children, and it’s really only a problem in pregnant women who contract it during their first trimester.
And, the thought was that, “Well, vaccinating for rubella is going to protect these pregnant women, and so therefore it’s morally justifiable.” But, in a situation… probably pretty analogous to the situation with COVID, when you look at the actual numbers that’s not the case. Because, prior to introducing the rubella vaccine, there was approximately 80% herd immunity in the population for rubella. And 80% herd immunity is the threshold at which the disease doesn’t circulate particularly well. Obviously it still circulates, people will still contract rubella, but it doesn’t spread through the population like wildfire and put lots of people at risk.
So, after using the rubella vaccine, what we now have is roughly 80 to 85% herd immunity. And so, you might say, “Well that’s a little better, so maybe it was worth it.” But for the first 10 years after this vaccine was introduced, there wasn’t a decrease in the cases of congenital rubella syndrome. And in fact, in the first few years after it was introduced, there was a spike in the cases of congenital rubella syndrome, they went up. And they didn’t start dropping until abortion became legal. And, there’s a pretty good case to be made that the drop in congenital rubella syndrome babies was due to their mothers being informed, “You have rubella, your child is likely to develop congenital rubella syndrome, why don’t you just abort it and try again.” The drop that we saw in that disease is probably a lot more due to elective abortions than it is to the introduction of the vaccine.
So, now we’ve got this vaccine that we have, I believe, worldwide. There’s 70% uptake of the MMR vaccine, which is the only way you can get vaccinated for rubella. You used to be able to get the vaccine separately, but Merck lumped them all together in the 1990s after the Wakefield scare, that potentially implied that the MMR was connected with the development of autism. And so, Merck just stopped producing the separate vaccines, you can only get it now as the trivalent vaccine with measles, mumps and rubella. Which means that you can’t ethically be vaccinated for any of those things because the vaccine is produced in aborted fetal cells. It’s produced in the WI-38 cell line, and that cell line took, I believe it was 32 abortions before they got to that cell line. The number 38, again, is the number of experiments that were actually performed, I believe it was 32 individual babies.
And then the virus that’s used in the measles vaccine, the attenuated measles virus, instead of just swabbing the throat of a sick child like they did in Japan, US researchers encouraged women who had been exposed to rubella in their first trimester to electively abort their children. They dissected 27 fetuses before they had the virus that is currently in use in the rubella vaccine, and they continued with 40 more elective abortions, isolating a number of different viral strains that didn’t ultimately get used in the vaccine. But, if you put all that together, you end up with approximately 99 abortions just for the rubella vaccine.
And keeping in mind that all of them are probably done under the same horrific conditions that we’ve just described, and in some cases where babies were delivered… the entire amniotic sac was removed from the mother and these babies were either dissected right then and there. And some cases they were stuck in the refrigerator to preserve them slightly so that they could be dissected in a little bit later, the brutality of that and the horror of that is not something that we should gloss over. Yet, your average Catholic parent who goes into the doctors office and is asked, “Do you want the MMR?” Doesn’t even know that this is how this was developed.
And so, when Bishop Schneider was talking in the interview he did with you about the moral complicit-ness that’s being asked on this grand scale of people to just accept this… this isn’t something that’s brand new with the advent of COVID, there’s already been significant inroads, I think, made in terms of getting people to appropriate evil to use something that has a truly evil origin for their benefit, even though they’re not really cooperating in bringing the evil about per se. And that doesn’t even get into the fact that continuing to do this then fuels the market for additional cell lines and additional aborted fetal products, and additional vaccines that are made in aborted fetal cells. Because, if we had been refusing the MMR vaccine, we wouldn’t have COVID vaccines that are made with aborted fetal cells. That would not have happened.
JHW: I have so many more questions for you I don’t know where to start. Let me go, first of all, to get to what you already said. What specifically did the PAV have wrong when they looked at the science, and what were they lacking?
PA: So, they were lacking an understanding of whether the vaccine was even protective or not. So, vaccines in general do have a modest protective effect against the disease that they’re trying to prevent, but implementing a vaccine doesn’t necessarily just tremendously impact herd immunity that might already exist in a population. And in fact, the chicken pox example is a great example of how disastrous the introduction of a vaccine can actually be to herd immunity. Because, what we’ve done by vaccinating everybody for chicken pox now is effectively eliminate the natural boosting cycle.
So, my parents got exposed to chicken pox again when I was a child and I got infected with the virus, and so their immune system was given a natural booster to say, “Hey, remember me? I’m the chicken pox virus. Why don’t you beef up your immune response a little bit so that you don’t develop shingles in a few years?” Because it’s caused by the same virus, and once you have the virus it does hang out in your nerve cells, and so if you’ve had chicken pox you can develop shingles. But, you don’t tend to develop it until a lot later in life because of this natural boosting process. Well, we’ve eliminated this in the population now, so we’ve basically pushed the average age of shingles lower, so we’re seeing more incidents of shingles, we’re seeing it in younger people. And we’re even seeing it in very young people who’ve been vaccinated for chicken pox. Because, the live attenuated virus that’s used in the vaccine also hangs out in your nerve cells and it can come back later as shingles itself.
So, one of the things that was missing from the Pontifical Academy of Life, in their determination here, is that you can’t just say, “Vaccines save lives, therefore this vaccine is a great idea.” You have to look at vaccines on a case-by-case basis and see if they’re justifiable. And the ones that are using aborted fetal cells, generally speaking, are not, they’re not really life saving vaccines, and so, you don’t really have a grave matter. Because, in order to participate in remote evil licitly… and as Bishop Schneider made a great case for, we’re sort of muddying the waters by even saying that we’re remotely participating in evil because the evil of abortion is so intense. But even if it were, the origin is extremely grave, you have to have extremely grave cause in order to actually make it licit. And so, they did not look at the science enough to see that the cause was just not proportionate.
And I think the same thing is true with the COVID vaccines, the cause is simply not proportionate. We’re looking at a death rate from Coronavirus, I think it’s .2% and the average age of death of a patient who is coded as having died from COVID… because there’s some question about whether patients who have comorbidities should even be counted as COVID deaths. The average age of these patients who are being said to die from COVID is around 79 to 83 years old, and the average life expectancy in the US is around 78.7 years. So technically, the average age of a COVID death is higher than the life expectancy in the US.
So, this disease isn’t really killing people right and left that weren’t probably going to die within [inaudible 00:33:15] anyway. It’s remarkable to me that anybody could consider this grave cause.
JHW: Many people think that when they’re taking a vaccine, “There’s nothing really of aborted babies in them, nothing really… it was tested on it, and it’s so remote, there’s really nothing there. If there is something even so remotely connected it’s like one billionth of a particle in the whole vaccination shot you get.” Speak to that for a second, if you would.
PA: With the Moderna and Pfizer vaccines there isn’t any aborted fetal material remaining in the vaccines because they’re not actually cultured or produced directly in the aborted fetal cells. But with the AstraZeneca vaccine and the Johnson & Johnson vaccine for COVID, as well as the rubella vaccine and the chicken pox vaccine, there are remainders of these aborted fetal cells that end up in the vaccines themselves. So, when you get this vaccine, you are actually injecting pieces of this individual who was murdered into your body. And those pieces tend to be remnants of DNA and some protein debris.
But the DNA is particularly of concern, because Dr. Theresa Deisher of Sound Choice Pharmaceuticals, which I think came into existence in the early 2000s. They were also working on solving this problem with ethical vaccines and the availability of ethical vaccines. she has some tremendous work, a lot of it she’s summarized in talk on YouTube, where she has looked at the relationship between the increase in use of aborted fetal cell derived vaccines, that corresponds to an increase in autism rates in the countries that she’s looked at. And, this has been in some countries in Europe as well as the United States. And she’s seen that there’s a dose dependent response, so the more aborted fetal cell vaccines that we use, the increase there is in incidents of autism.
So, she said, “Let’s take a look at that, let’s see if there’s any biologically plausible mechanism for that.” And so she made the connection that when you put these aborted fetal DNA contaminants into a living human being, something can occur… and this does occur in vitro, in cell culture in the laboratory, called homologous recombination, where the DNA that’s being injected into the individual can kind of line up with the DNA that it corresponds to in those individual cells, and then there’s some enzymes that can come along and they can swap those two pieces out. So, you end up losing your actual DNA and having the DNA from the aborted fetal cells incorporated into your cells.
And she was saying how this could potentially explain why in some individuals with autism… although not all because autism is a very multifaceted problem and there’s no one strict straight answer for why it develops in some individuals and not in others. But, in some individuals you see hundreds of what are called De Novo Mutations, so these are mutations that came out of nowhere, their parents didn’t have them, and you shouldn’t see hundreds of mutations in a child just from one generation. This child is very young probably still as well, they can’t possibly have accumulated all these mutations. Well they can, if this mutated DNA… because if you recall from back at the beginning of the talk, we talked about how in order for cell lines to be immortalized, we’re sticking viral oncogenes in them, these cancer promoting genes, these mutations into them in order to keep them growing in cell culture, somewhat indefinitely. The DNA in these cells has definitely mutated, so this could be the source of the mutations that we’re seeing in some of these kids that are developing autism.
So, this is one possible mechanism for why we’re seeing that. And it’s not outside the realm of possibility biologically, but also it makes sense if you think about it, just from natural law. If you’re going to do something as heinous as inject into yourself the remains of somebody who was murdered, there’s going to be a natural consequence to that. You can’t just do that and not have any negative effects, if that makes sense.
JHW: Well, we’re definitely into the safety portion of the discussion. And I’d really like to go right into that, especially with regard to what we’re seeing right now from some of the people who have already taken the COVID vaccines, either strain of them. We’ve seen a nurse come out with saying that one side of her face… she was experiencing Bell’s palsy, she seems to be paralyzed in one side of her face. We had one nurse take it early on and pass out. We had another doctor take it and apparently die. Could those be related to the vaccine? And what are some of the other safety concerns with the COVID vaccines, the ones that are approved and the ones that are awaiting approval now?
PA:
One of the main safety concerns with any of the COVID vaccines that are in development, is that most of them are what is called Nextgen technologies. These are things that have not been done in vaccines in the past, so we really don’t know how the mRNA vaccines, we don’t know what kind of longterm health effects they’re going to have. We don’t really know what effects they’re going to have in the body even short term. Because, one of the concerns that I have just from thinking about genetically engineering vaccines, way back in the late 90s when they were trying to have these fruits produce vaccine antigens and produce them in appropriate doses. When you would genetically transfect a plant and try to get it to produce, say smallpox antigens, they had a huge problem standardizing the dosage, and this is why the technology eventually got scrapped. Because, they simply couldn’t say that, “If you ate one banana then you’d get this much smallpox antigen.” Because all the bananas were different. And, bananas are maybe a bad example because bananas are polyploid and so there’s some other genetic problems going on there. But none of the plants that they tested were able to be standardized in terms of dosage.
So, when you insert foreign genetic material… and this is just true with the laboratory too. But when you insert foreign genetic material into a living organism, you can’t really control exactly how much protein that organism is going to produce based on how much DNA that you give it. And you can sort of guesstimate a range, but when you’re dealing with something like the SARS-CoV-2 spike protein… and we know that one of the ways that the pathology and the people who do get really sick is mediated, is through this overactive immune response. You get the cytokine storm, you get everything so amped up that your immune system is actually what’s killing your body. We’re going to then take genetic information, stick it into your body, not know how much protein you’re actually going to produce that causes this overactive immune response, and just say, “Oh yeah, you’ll be fine, don’t even bother to call me if you have some soreness in your arm.”
To me that’s mind boggling, because I don’t think they have any idea how wildly different peoples responses to this genetic information might be, and thus how wildly different their responses to the vaccine might be. And so, in addition to this general concern, there’s also the AstraZeneca and the Johnson & Johnson adenovirus vector vaccines. So, the idea is that we’re taking an attenuated virus that normally infects humans, which is adenovirus, and packaging some genetic information in there. And so, that virus vector is going to take that DNA from the Coronavirus to your cells and then put the DNA into your cells. And then at that point, you have even more possible complications because now not only are you sticking genetic information from Coronavirus into your body, but you also have the problem of… with adenovirus’ there’s… and I don’t remember the technical name for it, but there’s basically a mechanism whereby adenovirus’ can recombine in your body.
So, if you happen to be infected with an adenovirus, which may not even be symptomatic, because some of these viruses are very benign and they don’t really cause a whole lot of problems. But some of them are worse and they can cause common cold type symptoms, they can also cause digestive distress, things like that. But, say you’re infected with one of these adenoviruses, you get stuck with an adenovirus vaccine, and those two viruses, the vaccine virus and the wild-type virus, they actually recombine in your body and they make something different that we have no idea what it’s going to do, or how it’s going to react, or how it’s going to infect you.
And you can actually end up creating super viruses. And this is one of the reasons that when Coronavirus vaccines were originally being developed, back when SARS was a thing in 2003, 2004, they looked at doing live attenuated viruses. But then they said, “No, we can’t do that because you could have this live attenuated vaccine virus recombine with a naturally occurring Coronavirus.” Because there’re about four that normally infect human beings and cause common cold type symptoms, that’s not counting the SARS virus and the MERS virus, and the current SARS-2 virus. But, these four common ones could recombine with an attenuated live vaccine virus, and that could create something that we wouldn’t have any idea of how infective or how pathogenic it was. So, this is a concern I think too with the adenovirus factors that hasn’t been addressed properly in the public eye.
And then, one of the other things that I found interesting, I was looking at another video that was promoting these next generation technologies and how exciting they were, “Everybody calm down, we’ve been working on these for decades now, and they’re not just out of the box brand new, somebody just thought of this.” And as a researcher, hearing that, “We’ve been working on these for decades.” Doesn’t mean they’re safe, it means we haven’t had success in decades on this stuff. That’s the actual real message that’s being spun in a positive way, it’s like, “Oh, we have experience with this in a laboratory.” We have experience with it not working, is what we have.
JHW: So, one of the things that happens is, I think most people know but maybe you can address this very quickly, is that the companies that have produced these are indemnified against being sued. So in other words, if someone gets something from the vaccine, it’s the tax payer that’s going to deal with it, not the company. Yet the company is going to get profits from their making of it anyway, and got profits from their development of it because they were asked to do it under Warp Speed and with millions and billions of dollars. So, there’s that, and that fact that… well, maybe address that first. And then I have another question for you in a minute.
PA: So, that’s actually… minus the Warp Speed pre-funding, that’s actually the situation for all vaccines that are developed in the US. All vaccine manufacturers are indemnified against liability for their products, and it’s the Vaccine Injury Compensation Program, the VICP, that will deal with any claims of vaccine injury. And, I did talk about this a little bit in my book as well. And just crunching some numbers based on the actual number of adverse reports that are actually submitted to VAERS, which is the Vaccine Adverse Event Reporting System, based on the fact that that is probably much, much lower than what actually occurs. Because most people don’t, A, don’t think to file something, B, don’t file something because they know that it’s impossible to have it temporarily connected, or C in some cases, have know idea that there is a connection to the vaccine.
Because a lot of the adverse events that I talk about in the book is being very commonly or possible associated with vaccines, are very difficult to pin down in terms of their actual chronology, their development, their onset. Because a lot of them are allergic or autoimmune responses because you’re inciting your immune response in a very bizarre way actually. When you vaccinate yourself you’re not exposing yourself to the pathogen through the normal route, you’re going through your muscles instead of through your mouth. You’re in some cases giving yourself three, or four, or five or ten diseases at the same time. You would never as a child have measles, mumps, rubella, polio, chicken pox, diphtheria, tetanus and pertussis all at the same time, but you might get all those vaccines at one doctors visit.
So, there’s a lot of problems in terms of determining just how many adverse events there are associated with vaccines in general. But the vaccine manufacturers are not liable, and I think there’s going to be… there’s been some sort of special protections extended specifically for the COVID vaccines. Because, if you do obviously rush something to production, I think there is some sort of liability that you might still have, even as a vaccine manufacturer in general. But because this is now an emergency situation where you’ve been licensed to go ahead and do that, and cut your testing down to… I learned today that Moderna, they solicited adverse reactions for seven days. And I also learned today, that because it’s not considered ethical to not give somebody a Coronavirus vaccine if we have a ‘working’ Coronavirus vaccine, Pfizer is already vaccinating their placebo group with actual active vaccine.
So, we’re not going to have anymore data about longterm effects from these vaccines, because we’re not going to have anymore placebo group, because they’re going to go ahead and get the vaccine. Which, is mind blowing to me as a researcher and it’s just… how do you commit that level of… it’s scientific fraud, really truly, to just say, “We’re just eliminating our control group. We’re just completely taking them out of existence, so now we have no way to say how safe this vaccine is in longterm studies.”
JHW: One of the other things I meant to ask you, which follows right on what you just said, that is, the connection from when you take the vaccine to when you experience the effects isn’t immediate. It’s not like what we saw with the [inaudible 00:48:15]… what are we talking here? Is it a day, or two day? Or what is it?
PA: Well, it depends on the kind of reaction that you see. If you have anaphylaxis, which is a reaction that occurs with some vaccines, that’s the allergic response where your airways start to closeup and you’re in danger of dying from a severe allergic reaction. That happens, supposedly, approximately one in a million doses of your average vaccine. It happens 22 times more frequently than that with the COVID vaccines, so it’s one in 45,000 I think. Which is again, not a terribly, terribly high rate, but it’s 22 times more than your average, normally developed vaccine. And that should be frightening, because if people are experiencing anaphylaxis, which is the most severe possible reaction you could experience from a vaccine, 22 times more than they’re experiencing it from your average vaccine, what’s that say about other adverse side effects?
And so, you mentioned Bell’s palsy as one of the adverse side effects. We’re seeing Bell’s palsy, with both the Pfizer and the Moderna vaccine, they saw that more frequently in the vaccinated population than in the un-vaccinated population. Of course everybody wants to downplay it and say, “Most cases of Bell’s palsy resolve within six months.” But not all do. And the loss of facial muscle control isn’t always Bell’s palsy, it can also be symptomatic of other more problematic neurological disorders. Like Guillain-Barre syndrome, which everybody is quick to say, “We haven’t seen any cases of Guillain-Barre syndrome.” Well, how long have you tested for adverse reactions, 28 days? I don’t know if you’re going to see Guillain-Barre syndrome in 28 days, that’s one that takes longer to develop. So, autoimmune conditions, as a general rule, take longer to develop.
And there’s some evidence that type-1 diabetes is a possible side effect of vaccination. That can take a year to fully develop, once your body starts attacking your pancreatic cells. [inaudible 00:50:14] can take a really long time to develop. Fibromyalgia can take a really long time to develop.
But then other things, the most common severe adverse reactions, at least for the Moderna, seven and a 7.5 or 8% of people experience fatigue that’s severe enough to keep them from going about their average everyday activities. And I think about 6% experience headaches that are that severe. And there were a couple of other things that people were experiencing [inaudible 00:50:44] that would happen within a day or two, or even immediately of the vaccine. So, just depends on the adverse reaction.
The stuff that I’m most worried about is that chronic, longterm downstream stuff. And I have a vested interest in this because my family has very interesting case history of all kinds of autoimmune problems, from my grandmothers generation on down to my sisters children. And, whether these are all associated with vaccines or not, I can’t say, and I certainly don’t think my grandmothers generation was probably the case because they weren’t receiving very many doses back then. But I do know, that if vaccines can trigger autoimmune pathology, and I clearly have the genetics for autoimmune problems, I’m not taking an unnecessary vaccine, that’s just not intelligent. But that’s the part that concerns me the most, because those things aren’t going to show up until we’ve already vaccinated who knows how many people. If it’s going to take six months to a year, to several years for this pathology to really develop, and then it’s very hard to tie it back to the original vaccine in some cases.
JHW: The UK government has warned pregnant women not to take it. The FDA and other agencies have warned that those with allergic reactions to vaccine ingredients shouldn’t take it. There was a warning that men might consider freezing their sperm before taking it because of some kind of fear of possible effect that way. What have you known of those possibilities and things like that? Is this a concern for fertility as well?
PA: I would love to be able to give you a definitive answer on that, and I can’t. And part of the reason I can’t is because there is a lot of conflicting information that’s being circulated. And even with the expertise that I have, I haven’t been able to make sufficient heads or tails of it to be able to say one way or the other. I will say that the British Government is issuing that warning in part, because there hasn’t been any testing done in pregnant women. So, you don’t give a vaccine to a susceptible group that there’s no safety testing on, generally speaking, is the thought there. I don’t think that’s being done out of a motivation of they know something about fertility that they’re not saying, they’ve come out and said, “There’s been no testing done, so we shouldn’t do this.”
But there was some information that was circulated that was saying, “Don’t get it if you’re planning to be pregnant within the next couple of months.” Which seemed very strange to me, because that’s not something that’s issued with your average vaccine. And if it does cause fertility issues, it certainly wouldn’t be the first vaccine to cause fertility issues.
There’s been a number of vaccines that the Word Health Organization has had in development that were on purpose supposed to cause infertility. They’ve been looking for a birth control vaccine since the 1970s. They have tested uninformed, non-consenting women in Kenya, and the Philippines and Mexico, and I believe a couple other third world countries. And I actually have spoken personally with a doctor in Kenya, who was one of the ones who identified that the tetanus vaccines that were being administered to Kenyan women, and we specifically being targeted to women of childbearing age, were laced with hCG. Which, if you inject that in conjunction with tetanus toxoid, you can render women infertile for an indefinite period of time. So, this is something that has been done in the past, covertly, and I think that’s part of the reason why a lot of people are really concerned.
And then Gardasil, the HPV vaccine, is associated with a frightening drop in fertility. And there’s a study done on women, I believe, aged 25 to 29 who had or had not received the vaccine, so this wasn’t a trial that was done, it was just looking at data afterwards. And, women who had received all three doses of he HPV vaccine were one third as likely to have conceived and borne a child as women in the same age cohort, roughly adjusted for other medical issues that could possibly effect fertility. You had three times as much likelihood of being pregnant if you had never had the vaccine, versus if you’d had all three doses. This is alarming stuff, because you’re not told this…
JHW: Absolutely.
PA: … when you go in and your doctor says, “Would you like your daughter to get Gardasil?” You’re not told she might develop these horrible autoimmune diseases that have been associated with it, including chronic fatigue syndrome and a syndrome called PoTS. And I can never remember what PoTS stands for, but it’s horrific to have it, I know some individuals who do and it’s very limiting for them, it’s a heart condition. And then, you’re also not told, “And P.S. you might also never be able to conceive a child.”
JHW: Let’s touch a little bit more on whether this vaccine for COVID is necessary, and then after that I’ll ask you to give some final thoughts.
PA: Did you have a specific question about that or just in general?
JHW: One of those considerations, when you look at vaccines, is about whether it’s needed or not. We talked about the safety, we talked about the morality, we talked about the effectiveness, but is it actually needed? And that looks at what our current situation is with COVID right now.
PA: We talked a little bit about the death rate, the death rate is very, very low. The average age of death is higher than the average expected mortality in the US. We’re not in a position where it seems necessary, and the safety concerns seem to even offset the benefits, in terms of I think you’re more likely to have an adverse reaction to the vaccine then you are to catch COVID, let alone to die from COVID. But also, nobody has claimed… or they very cleverly just not mentioned it while trumpeting other areas of success, but nobody has claimed that [inaudible 00:56:41] of the vaccine will actually cause the virus to stop spreading. The only claims that have been made by both Pfizer and Moderna is that, “If you get the vaccine, you’re less likely to get severe COVID symptoms than if you don’t get the vaccine.” And again, they’re looking at a fraction of the cohort that they vaccinated.
So, Pfizer vaccinated 43,000 people and they looked at approximately 200 people who developed symptoms. And then Moderna, same thing, vaccinated 30,000 people, looked at approximetely 200 people who developed symptoms. And then they both made claims that their vaccines were 90 something percent effective, based on the fact that, “Well, the people who developed symptoms, 90% of people who developed the worse symptoms, were in the un-vaccinated cohort.” They didn’t test for whether these people were positive for SARS Coronavirus, they didn’t look at any other symptoms, they didn’t look at, “Longterm does this actually keep you from developing symptoms over a longer period of time?” And they looked over a period of just a couple of weeks, as we’ve said. They didn’t test any of the things that they should have tested, in terms of determining whether this vaccine is actually protective or not.
So, we don’t have any reason to believe that this vaccine would do anything to slow the spread of the virus. And very high profile people are saying, “Get the vaccine, get the vaccine, but keep wearing your mask because it’s not actually going to effect transmission.” Why then why am I getting the vaccine?
JHW: Exactly. And how dare you suggest that in order to travel, in order to make society come back to normal, need a vaccine, because then that makes no sense whatsoever.
PA: The only reason I would get the COVID vaccine is for my own benefit for that modest, protective effect against developing the worst possible symptoms. For me, I’m not in a high risk cohort, I don’t have comorbidities, there’s no reason for me to get that vaccine, it’s not going to help my neighbor. It’s not ‘the right thing to do’ or the moral thing to do, or a necessary thing to do for anybody other than myself. And, if it’s not necessary for myself, then it’s absolutely unnecessary for me to get this shot.
JHW: Pamela, just before I ask you for your final thoughts before we end off, I wanted to thank you on behalf of all of our LifeSite viewers. I know a lot of people have been asking questions, and I have got from you clearer answers than I’ve ever seen anywhere before, so thank you for that. Your book called Vaccination: A Catholic Perspective, is available where?
PA: It’s available on the Kolbe Center’s website, so that’s Kolbe like [inaudible 00:59:21], K-O-L-B-E, C-E-N-T-E-R dot org.
JHW: We’ll be linking to it in my blog post and in the description of this video as well. But, give us if you would Pamela, your final reflections on this question.
PA: The short thing is don’t get it, it’s not good for your soul and it’s not good for your body. And I think that we really need to, as Catholics, if we don’t stand up now… we’re losing the opportunities we’re ever going to have to stand up and rectify this wrong that’s been going on now for decades. And it’s been going on for decades and we’re going to be accountable for that. We lived in this time, we had an opportunity to stand up, we had an opportunity to do something, and if we don’t, we are going to be held accountable for that at the end. You can’t just sit on your hands and say, “Oh well, I’m not going to take it. Oh well, it’s not that big a deal.” This is a big deal, this is a hill worth dying on.
JHW: Amen. And you have very, very providentially been given to do this work, to start it before it was so evident that it was so extremely needed, and it comes out now as if planned. May God bless you for what you’ve done and the clarity that you’ve brought.
PA: Thank you very much.
JHW: And God bless all of you. We’ll see you next time on the John-Henry Westen show.